|
ADS
Place your advertisement
here.
Email
info@centerltc.com
or call Damon at 206-283-7036 for advertising rates.




American Independent Marketing




Join the Center for Long-Te Care Reform.
Help us fight for rational LTC policy reform.
Receive our daily email publications.
Get a user name and password to our Members-Only Zone.
Only $150 per year.
Mail your check to Center for Long-Term Care Reform, Inc., 2212 Queen Anne
Avenue North, #110, Seattle, Washington, 98109.
Contact Damon at 206-283-7036 or
damon@centerltc.com
if you have questions. Join
the team!
|

READ STEVE'S BIO.JPG)
#############################
Updated Monday, August 10, 10:03 AM
(Pacific)
Seattle—
#############################
LTC
E-ALERT #26-028: LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
CareScout Redefines Worksite Long-Term Care
Insurance With a Solution That Goes Further for Employers and Employees
-
Senior care and living sector outperforms others in
real estate for seventh quarter in a row
-
Providers tap new AI tools to minimize managed care
requests and denials
-
The Facts About Medicare Spending
-
How CMS Can Restore Program Integrity to Medicaid
by Eliminating Passive Redetermination Requirements
-
Lumos Insurance Introduces the Immediate Care Plan
to Help Families Fund Long-Term Care
-
Can You Actually Get Paid to Care for an Aging
Parent?
-
Ownership changes, regulatory and reimbursement
pressures top reasons for nursing home closures, study finds
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Friday, August 7, 2026, 10:03 AM (Pacific)
Seattle—
#############################
LTC BULLET: PARAGON ON
MEDICAID AND LONG-TERM CARE
LTC Comment:
Paragon Health Institute, America’s
leading health policy think tank, brought Medicaid and LTC inequities to
the Senate Budget Committee’s attention this week. The
hearing video is captivating. We
elaborate after the ***news.***
*** 8/4/2026, “Lumos
Insurance Introduces the Immediate Care Plan to Help Families Fund
Long-Term Care,” StreetInsider.com
Quote:
“Lumos
Insurance™ today announced the general
availability* of its Immediate
Care Plan, a fully underwritten single
premium immediate annuity built for people who already need paid care. A
single lump sum is exchanged for guaranteed monthly income for life, with
payments beginning within one month, so families can fund an assisted
living community, a memory care unit, or in-home care without drawing down
every other asset they have. … The Immediate Care Plan addresses what
Lumos calls the Care Gap: the recurring difference between the monthly
cost of formal care and the income a family already has coming in
from Social Security, a pension, or other sources. … ‘The Care Gap is
showing up in advisors' offices every week, and without a solution, it can
put a lifetime of savings at risk,’ said Vince Bodnar, President of Lumos
Insurance and a two-time chairperson of the Society of
Actuaries' Long-Term Care Insurance Section. ‘When a product is priced for
the average person instead of the individual, families may commit more
assets than their situation requires. The families arriving at the care
transition today deserve solutions built for their actual circumstances —
not actuarial averages. Lumos is excited to offer our Immediate Care Plan
to help meet this need.’”
LTC Comment:
Congratulations to Center-corporate-member Lumos and its president Vince
Bodnar on the introduction of this promising new solution to a
longstanding problem for LTC consumers. ***
LTC BULLET: PARAGON ON
MEDICAID AND LONG-TERM CARE
LTC Comment: Paragon
president Brian Blase described the hearing and his testimony in the
Institute’s
weekly newsletter:
“Medicaid:
The Reality” was the first Senate Budget
Committee hearing under Chairman Ron Johnson’s leadership. My oral
testimony focused on Medicaid’s
fundamentally broken financing incentives. I explained that the ACA
created a financing formula that pays states roughly $9 in federal funds
for every $1 they spend on able-bodied, working-age Medicaid expansion
adults, compared to an average of $1.33 for every $1 spent on traditional
enrollees. That sevenfold disparity encourages states to prioritize
expansion adults over the populations Medicaid was originally created to
serve—and has resulted in worse health care access for traditional
enrollees. I also described how provider taxes, state-directed payments,
and other financing arrangements have evolved into a legalized Medicaid
money-laundering apparatus that shifts costs from states to federal
taxpayers while generating tens of billions of dollars in corporate
welfare for politically powerful providers, insurers, and consultants.”
Do yourself a favor and
watch this video of the full hearing: “Medicaid:
The Reality” . It is engaging and
informative, but for pure entertainment value, check out
the exchange between Senator John Kennedy and Brian Blase.
Also of interest, testimony by Jonathan Ingram, Vice President of Policy
and Research at the Foundation for Government Accountability, concerning
Medicaid’s excessive improper payments. The third witness at the hearing,
Mr. Andy Schneider,
Research Professor of the Practice Center for Children and Families,
McCourt School of Public Policy, Georgetown University, is a study in
hapless defense of Medicaid’s dysfunctions in the face of hard, empirical
evidence of their damage.
But you might ask: What
does this have to do with long-term care? ObamaCare’s (ACA’s) expansion
population generates 90% federal matching funds for state Medicaid
programs when they cover able-bodied, working age adults. At seven times
the match for poor women, children, the aged, blind and disabled (ABD),
this distorted incentive moved Medicaid funding away from the program’s
traditional, more vulnerable enrollees. For example, ABD recipients were a
quarter of total enrollment in 2010 (when the ACA passed) and they
consumed nearly 2/3 of all Medicaid expenditures. By 2025, ABD recipients
were down to 1/5 of total enrollments and they accounted for only half of
total expenditures. This ABD population consumes the majority of LTC
benefits—including nursing facility care and home and community-based
services (HCBS). LTC alone accounts for approximately one-third (30% to
33%) of all Medicaid spending, despite being used by only 6% of total
Medicaid recipients who are mostly ABD. Prioritizing able-bodied, working
age adults over Medicaid’s original target population of those most
vulnerable and in need has changed the program’s focus from helping those
with the greatest need into a non-tax federal money generator for states.
More on Long-Term
Care
Congressional hearing
testimony generally takes the form of brief verbal statements by witnesses
who also submit much more detailed written testimony. Most interesting to
us is that Brian Blase’s written testimony included the following content
close to our hearts. By highlighting the problem of excessive use of
Medicaid LTC by people who could, should and would have paid their own way
and stayed off Medicaid, Blase pointed the way toward better policy to
benefit both the poor and the more affluent.
The following is a quote
from Brian Blase’s
written testimony:
“MEDICAID’S DAMAGE TO
RESPONSIBLE LONG-TERM CARE PLANNING
“A fundamental flaw in
America’s long-term care system is that Medicaid has evolved from a safety
net for the poor into an inheritance protection program for many
households with substantial assets. Through generous asset exemptions,
home equity exclusions, trusts, and estate-planning strategies, many
individuals can qualify for taxpayer-financed long-term care while
preserving significant wealth for their heirs. Rather than requiring
families to use accumulated assets to finance their own care before
relying on public assistance, current policy often allows Medicaid to pay
first while inheritances remain largely intact. This is inequitable to
taxpayers who save responsibly and distorts the program’s original
purpose.
“These policies also
create powerful disincentives for individuals to prepare for their own
long-term care needs. When people expect Medicaid to cover nursing home
costs or home-based care after modest planning or asset restructuring,
they have less reason to purchase long-term care insurance, accumulate
dedicated savings, or otherwise plan for a predictable risk associated
with aging. The result is a classic moral hazard: private financing
declines because public financing is readily available. As more people
rely on Medicaid, the program consumes more taxpayer resources while
providers become increasingly dependent on low Medicaid reimbursement
rates, contributing to workforce shortages, limited access to high-quality
care, and persistent financial pressures throughout the long-term care
system.68
“The irony is that these
policies often harm the very people they are intended to help. By
encouraging reliance on Medicaid rather than personal planning, they
weaken the market for private long-term care financing and reduce the
resources available to improve care quality for the most vulnerable. A
system that requires individuals with sufficient means to finance more of
their own long-term care before turning to Medicaid would better preserve
the program for those with genuine financial need while encouraging
greater personal responsibility and a stronger private market for
long-term care services.
“III. Recommendations
to Improve the Medicaid Program …
“Reform
Medicaid long-term care
“Medicaid should not be
used to preserve inheritances for wealthy heirs. Congress should ensure
that people with sizeable assets are not able to use Medicaid to finance
their long-term care expenses.
“These reforms will
reduce waste, fraud and abuse and provide Medicaid a responsible fiscal
trajectory to ensure we continue to have the ability to care for our most
vulnerable.”
68
Stephen Moses, "Long-Term Care: The Problem," Paragon Health Institute,
October 2022, https://paragoninstitute.org/medicaid/long-term-care-problem/
LTC Comment:
My role as a
Visiting Fellow with the
Paragon Health Institute has widened the
reach of the Center for LTC Reform’s research and analysis through
numerous reports and articles for
Paragon.
#############################
Updated
Monday, August 3, 10:03 AM (Pacific)
Seattle—
#############################
LTC E-ALERT #26-027:
LTC NEWS AND COMMENT
LTC Comment: Do you
spend hours searching the internet for useful articles, key data, and
relevant reports to keep you on the forefront of professional knowledge?
Do you lose business because you’re blindsided by clients or competitors
who learn critical information before you do? Here’s an antidote:
LTC Clippings: The
Center for Long-Term Care Reform notifies subscribers to our LTC Clippings
service daily of information you need to know. Each message contains only
the critical facts about new publications: a title, representative quote,
a link to the original, and our analysis in a sentence or two. To inquire
or subscribe, contact Damon at 206-283-7036 or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC E-Alerts: Once a
week, we compile our daily LTC Clippings into a summary, email it to
Center for Long-Term Care Reform members, and archive it in The Zone, our
password-protected members-only website. Center members also receive our
weekly LTC Bullet op-ed. To join the Center and receive all these
benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no longer post our
LTC E-Alerts on the Center’s public access website, but here’s what
today’s LTC E-Alert contained: links, quotes and comments on the
following articles, reports, or data:
-
How to make social
care sustainable
-
Federal Government
Spending Is a Leaky Bucket
-
New resource helps
senior living professionals share sector’s value proposition over
staying at home
-
The Retirement
Myth Everyone Gets Wrong About Medicare
-
The Medicaid Rule
That Can Put Your Family Home at Risk
-
Retirement-long
medical expenses increasing for older adults, cutting into savings
-
How Much Would A
Public Long-Term Care Insurance Program Cost?
-
As the cost of
aging soars, families’ wealth is evaporating
#############################
"LTC E-Alerts" are
a
feature offered by the Center for Long-Term Care Reform, Inc. to members
at the $150 per year level or higher. We'll track and report to you news
and analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Monday, July 27, 10:03 AM
(Pacific)
Seattle—
#############################
LTC
E-ALERT #26-026: LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Kansas City won’t escape the US debt crisis. Here’s
what we must do now
-
The Average Net Worth of Americans at 85, And The 8
Assets Separating the Comfortable From the Struggling
-
Rewarding Reform, Punishing Neglect: How Annual
Improper Payment Reviews Can Fix Medicaid Accountability
-
Managed care plan’s termination of assisted living
program leaves providers in limbo
-
Caregiver Burnout — Why Generic Advice Fails and
What Works
-
Older adults’ home equity reaches a record $14.92T
in first quarter
-
BREAKING: New exclusion authority expected to be
‘force multiplier’ for CMS fraud enforcement
-
Despite DOJ policy shift, state obligations to
people with disabilities remain
-
SNF occupancy hits highest level in a decade: NIC
-
Spouses of patients with dementia nearly 75 percent
more likely to develop same condition, large study finds
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Friday, July 24, 2026, 10:03 AM (Pacific)
Seattle—
#############################
LTC BULLET: LONG-TERM
CARE FRAUD
LTC Comment: LTC fraud
is large and growing especially in the public sector, which could learn
from the private sector’s better identification and control methods. We
announce a new Center report on LTC fraud, after the ***news.***
***
illumifin, the leading insurance third party administrator (TPA) and
longtime Center-corporate member, inspired and assisted our work on LTC
insurance fraud. The company’s excellent presentations on LTCI fraud at
the 2025 Intercompany LTC Insurance Conference last March pointed the
direction for our research. Executive Chairman Peter Goldstein encouraged
our study and Jeffrey Ferrand, Vice President of Fraud Services at
illumifin, provided helpful advice and suggestions. We thank the company
and its officials for the path-breaking work they’ve done to identify,
prevent, and prosecute the various forms of fraud confronting the
long-term care insurance industry. ***
LTC BULLET: LONG-TERM
CARE FRAUD
LTC Comment: Today, the
Center for Long-Term Care Reform published a new report titled “Long-Term
Care Fraud.” Its “Executive Summary” and “Conclusion” follow below but you
can check out the complete report
here.
Long-Term Care Fraud
by
Stephen A. Moses
July 23, 2026
Executive Summary
Health care fraud is
large already and growing rapidly. Long-term care (LTC), vital because of
America’s aging population, is especially susceptible to fraud. Government
or corporate third parties finance most LTC which creates a moral hazard
by facilitating fraud and reducing its risk. Individuals, naturally averse
to fraud, fund much less LTC out of their own pockets. Most LTC is
delivered in private homes without supervision inviting fraudulent
billings. We know the incidence and cost of fraud in private LTC
insurance. But there is no published measure of LTC fraud in the public
sector. Medicaid and Medicare present special problems that make LTC fraud
identification, processing and prosecution exceptionally difficult. The
Trump administration has undertaken a major push to reduce public sector
health care fraud. Private sector advances to control LTC fraud could help
reduce obstacles on the public side. A key is prioritization, focusing on
cases most likely to produce results. This paper examines LTC fraud in
both sectors and recommends measures to curtail its growth and impact.
…
Conclusion
LTC fraud is inevitable
in a health care system that relies heavily on third-party payment,
limited supervision, and complicated public administration. As demand for
LTC grows with population aging, the chances for phantom billing, upcoding,
identity abuse, and organized fraud expand unless payers respond more
aggressively. Private LTC insurers have identified and reduced fraud by
using targeted investigation, risk scoring, and early intervention instead
of waiting to recover losses after the fact. Public programs, especially
Medicaid and Medicare, face greater barriers, but they could employ the
most effective private-sector practices more aggressively. Focus on
high-risk claims; use data analytics to stop suspicious payments earlier;
and prioritize cases with the greatest return on investigative effort. In
a system where most LTC spending comes from third parties, fraud control
will always depend on incentives. Replacing Medicaid’s wide open federal
funds matching system with capped block grants would encourage states to
focus more vigorously on fraud control. Absent the temptation of unlimited
federal revenue, state Medicaid programs would more effectively protect
vulnerable recipients, preserve public funds, and maintain trust in
long-term care.
#############################
Updated
Monday, July 20, 10:03 AM (Pacific)
Seattle—
#############################
LTC E-ALERT #26-025: LTC NEWS AND COMMENT
LTC Comment: Do you spend hours searching
the internet for useful articles, key data, and relevant reports to keep
you on the forefront of professional knowledge? Do you lose business
because you’re blindsided by clients or competitors who learn critical
information before you do? Here’s an antidote:
LTC Clippings: The Center for Long-Term
Care Reform notifies subscribers to our LTC Clippings service daily of
information you need to know. Each message contains only the critical
facts about new publications: a title, representative quote, a link to
the original, and our analysis in a sentence or two. To inquire or
subscribe, contact Damon at 206-283-7036 or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC E-Alerts: Once a week, we compile our
daily LTC Clippings into a summary, email it to Center for Long-Term Care
Reform members, and archive it in The Zone, our password-protected
members-only website. Center members also receive our weekly LTC Bullet
op-ed. To join the Center and receive all these benefits and more,
contact Damon at 206-283-7036 or
damon@centerltc.com.
We no longer post our LTC E-Alerts on the
Center’s public access website, but here’s what today’s LTC E-Alert
contained: links, quotes and comments on the following articles, reports,
or data:
-
HSAs undertapped
as way to save for long-term care, retirement needs, survey finds
-
Violence
repeatedly erupts in dementia care despite warnings, inspections show
-
My mom's long-term
care has cost almost $400,000. This is after we spent $45,000 converting
a guest house on our property for her
-
New study
quantifies the annual cost of dementia at $818 billion, with families
picking up most of the tab
-
[UPDATED] CMS to
reward higher-performing nursing homes with ‘streamlined’ reviews,
favorable online icon
-
Five Key Facts
About Spending and Enrollment for People with Medicare and Medicaid
(Dual-Eligible Individuals)
-
Report offers
roadmap for future-proofing care for older adults
-
Alzheimer’s
Association starts $100M trial to evaluate impact of GLP-1s on cognitive
decline
-
Baby boomers
retiring with record mortgage, credit card debt
-
Improving Access
to Medicare Home Health Care: Key Policy Considerations
#############################
"LTC E-Alerts" are
a
feature offered by the Center for Long-Term Care Reform, Inc. to members
at the $150 per year level or higher. We'll track and report to you news
and analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Monday, July 13, 10:03 AM (Pacific)
Seattle—
#############################
LTC E-ALERT #26-024: LTC NEWS AND COMMENT
LTC Comment: Do you spend hours searching
the internet for useful articles, key data, and relevant reports to keep
you on the forefront of professional knowledge? Do you lose business
because you’re blindsided by clients or competitors who learn critical
information before you do? Here’s an antidote:
LTC Clippings: The Center for Long-Term
Care Reform notifies subscribers to our LTC Clippings service daily of
information you need to know. Each message contains only the critical
facts about new publications: a title, representative quote, a link to
the original, and our analysis in a sentence or two. To inquire or
subscribe, contact Damon at 206-283-7036 or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC E-Alerts: Once a week, we compile our
daily LTC Clippings into a summary, email it to Center for Long-Term Care
Reform members, and archive it in The Zone, our password-protected
members-only website. Center members also receive our weekly LTC Bullet
op-ed. To join the Center and receive all these benefits and more,
contact Damon at 206-283-7036 or
damon@centerltc.com.
We no longer post our LTC E-Alerts on the
Center’s public access website, but here’s what today’s LTC E-Alert
contained: links, quotes and comments on the following articles, reports,
or data:
-
A New Option for Long-Term Care Costs
-
US adult obesity rate rose from 30% to 41% between
1999 and 2023, study finds
-
It’s Time To Reform How The Federal Government
Funds State Medicaid Programs
-
Genworth CEO McInerney takes health leave as CFO
Upton steps in
-
New tool helps providers, others estimate how long
someone will be able to afford assisted living
-
Collateral damage: Medicaid work rules threaten
nursing homes even if patients keep coverage
-
The families we serve are becoming the workforce we
need
-
Long-Term and Assisted Care—Here’s What Medicare
and Medicaid Do and Do Not Cover
#############################
"LTC E-Alerts" are
a
feature offered by the Center for Long-Term Care Reform, Inc. to members
at the $150 per year level or higher. We'll track and report to you news
and analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Friday, July 10, 2026, 10:03 AM (Pacific)
Seattle—
#############################
LTC Comment: If you
think LTC is in trouble now, wait until the rest of the boomers hit age 65
in 2029! We explain after the ***news.***
*** Did you see all of these important LTC stories
from the past few days? Probably not unless you track the industry media
and academic publications full time. That’s what Steve Moses does so he
can send these real time LTC Clippings to Center premium members
daily.
7/8/2026, “As
America Turns 250, It's Worth Celebrating Last Year's One Big Beautiful
Bill,” by Brian Blase, Paragon Health Institute
Quote: “Maximizing freedom requires limiting government. Last
year, Congress notched a win for freedom with the passage of the One Big
Beautiful Bill (OBBB), or the Working Families Tax Cut Act. Although the
cornerstone of the legislation was its provisions that lowered taxes, the
legislation also expanded freedom by taking steps to reduce the tide of
red ink emanating from federal health care programs, whose unsustainable
growth poses one of the greatest threats to America’s long-term
prosperity.”
LTC Comment: Have you seen the relentless media criticism of last
year’s budget reconciliation law? Read this excellent summary of the
OBBBA’s impact on government health care spending for a more accurate and
objective analysis.
7/7/2026, “The
Aging Population Is Changing States’ Revenue, Spending, and Service Demand
Outlook,” PEW
Quote: “The United States’ population is aging rapidly. And as
with other
long-term shifts in social and economic conditions, the transition to
an older population is already affecting state revenue and
expenditures. Understanding and preparing for these ongoing changes will
be critical to states’ future fiscal sustainability.”
LTC Comment: Read this report to learn now states are already in a
world of fiscal hurt due to population aging. Then contemplate how much
worse it will be without the ongoing federal Medicaid matching funds
bonanza as new limits on the use of provider taxes, intergovernmental
transfers, and state-directed payments take effect. No amount of planning
will shield states from what’s coming. Expect less government help for LTC,
not more.
If you’re not already a member of the Center for
Long-Term Care Reform, join
here. Check out our “Membership
Levels and Benefits” for all the individual and corporate membership
options. Join our campaign to ensure quality long-term care for all
Americans. ***
LTC BULLET: HOW MUCH
WORSE CAN LONG-TERM CARE GET?
LTC Comment: U.S.
long-term care (LTC) is in a world of hurt. The symptoms are well known:
access and quality problems, caregiver shortages, excessive reliance on
unpaid family caregivers, exploding public costs, and so on. Bad as it is,
however, evidence suggests it could, and likely will, get much worse.
Two articles in the
current issue of Health Affairs support that discouraging
conclusion. “National
Health Expenditure Projections, 2025–34: Strong Utilization Growth
Initially, Legislative Impacts Later”
tells us that the key components of LTC spending will grow annually on
average from 2025 to 2034 by the following percentages arriving at total
spending across all payers in billions of dollars as follows:
Nursing care facilities and
continuing care retirement communities:
4.4%, $338.3
Home health care:
8.1%, $367.8
Other health, residential, and personal
care: 6.7%, $615.0
OK, that’s bad enough
considering the 2024 numbers for the nursing homes, home health and other
categories were only $219.9, $169.4 and $320.5, respectively. But consider
how much worse LTC spending could get if the insights from the other
Health Affairs article are not adequately reflected in these
estimates.
According to “Trends
In Care Needs Among Older US Adults Diverged By Age, 2011–22,”
a new cohort of markedly more unhealthy baby boomers is about to throw
current expectations about LTC utilization and spending into a cocked hat.
For starters, consider
the status quo: “Nearly half of older adults in the United States
experience disability, often defined in later life as limitations with
daily activities … .” (p. 790) Half have ADL deficiencies? Already?
That’s alarming enough. But consider what’s coming according to the
“trends” article.
Among younger baby
boomers, “swelling numbers” are living with ADL limitations, receiving
paid care, and experiencing unmet care needs. Among older age groups,
however, there were declines in care received in all settings without
increases in unmet care needs. Overall, averaging the younger and older
cohorts, trends for the 65 and older population appeared stable with half
having ADL deficiencies.
But that current
stability is misleading. This study only analyzed the front half of the
baby boom generation. Future studies will address all the baby boomers and
will not be balanced by the better health and LTC characteristics among
the older cohort in the current study.
The trend article
authors conclude “the sizable rise in the numbers of adults ages 65–74
with activity limitations (an additional five and a half million),
receiving care (an additional three million), and with unmet care needs
(an additional two million) over a relatively short period is sobering.”
(p. 796)
“Sobering” is an
understatement. America’s over 85 age population will triple by 2050
dramatically increasing the number needing LTC. The article therefore
concludes:
Taken together, study
findings point to continued swelling in the numbers of older adults with
care needs as the second half of this generation reaches later life. They
also suggest that the share of older adults with care needs, which has
been flat for more than two decades, may soon begin to rise. (p. 796)
From its beginning in
1946, the baby boom generation dramatically transformed American society,
culture and economy. It’s about to shake up LTC services and spending
commensurately. The first tranche of baby boomers has more ADL
limitations, requires more paid care, and has more unmet LTC needs than
previous generations. Add in the younger boomers with LTC characteristics
as bad or worse and we can expect the LTC service delivery and funding
challenge to worsen radically.
So, what is to be done?
Do either of the Health Affairs articles offer helpful suggestions?
Alas, no. The projections article concludes “policy makers will
undoubtedly continue to explore options for addressing the significant
financing challenges for a sector that is expected to account for more
than one-fifth of the economy by 2034.” (p. 732) Want to hang our hopes on
policy makers finding a better funding source?
The trends article is no
more helpful. “Study findings reinforce the need for robust policies,
including innovations in workforce development and family supports, to
address the growing care needs of older adults and their families.” (p.
797) Where will the money come from to reinforce robust policies? That’s
typical doubletalk.
What these articles have
in common with most others of their ilk is that they analyze symptoms and
recommend solutions, but never ask why LTC is so dysfunctional in the
first place. With no idea of the source of LTC’s many problems, such
analysts have nowhere to go with their recommendations than to call for
more government spending and regulation.
For an entirely
different approach that addresses the cause of LTC problems first and then
proposes solutions, read the
Paragon Health Institute’s “Long-Term
Care: The Problem” and “Long-Term
Care: The Solution” and watch this “virtual
LTC event” featuring age wave visionary
Ken Dychtwald and leading LTC researchers. To find ample private funds for
LTC, check out “Medicaid’s
$100+ Billion Leak.” For what not to do,
see “Medi-Cal-amity:
California’s Reckless Expansion of Medicaid Long-Term Care to the Affluent.”
See also “Better
Long-Term Care for Billions Less.” Much
more on long-term care
here.
#############################
Updated
Monday, July 6, 10:03 AM (Pacific)
Seattle—
#############################
LTC E-ALERT #26-023: LTC NEWS AND COMMENT
LTC Comment: Do you spend hours searching
the internet for useful articles, key data, and relevant reports to keep
you on the forefront of professional knowledge? Do you lose business
because you’re blindsided by clients or competitors who learn critical
information before you do? Here’s an antidote:
LTC Clippings: The Center for Long-Term
Care Reform notifies subscribers to our LTC Clippings service daily of
information you need to know. Each message contains only the critical
facts about new publications: a title, representative quote, a link to
the original, and our analysis in a sentence or two. To inquire or
subscribe, contact Damon at 206-283-7036 or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC E-Alerts: Once a week, we compile our
daily LTC Clippings into a summary, email it to Center for Long-Term Care
Reform members, and archive it in The Zone, our password-protected
members-only website. Center members also receive our weekly LTC Bullet
op-ed. To join the Center and receive all these benefits and more,
contact Damon at 206-283-7036 or
damon@centerltc.com.
We no longer post our LTC E-Alerts on the
Center’s public access website, but here’s what today’s LTC E-Alert
contained: links, quotes and comments on the following articles, reports,
or data:
-
Data detail extent
of senior living and care provider reliance on immigrant workers
-
Sector challenges,
skilled nursing turnover present opportunity for first-time
entrepreneurs, ‘innovators’
-
BREAKING: CMS
unveils aggressive plan to fine, more easily expel noncompliant Medicare
providers
-
Lear's age of
suffering
-
Nearly Four
Million Medicare Beneficiaries Met the Eligibility Criteria in 2023 for
the Medicare GLP-1 Bridge
-
Medicare Advantage
by Default
-
Medicaid HCBS
growing, but worker wages falling, new study finds
#############################
"LTC E-Alerts" are
a
feature offered by the Center for Long-Term Care Reform, Inc. to members
at the $150 per year level or higher. We'll track and report to you news
and analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Monday, June 29, 10:03 AM
(Pacific)
Seattle—
#############################
LTC
E-ALERT #26-022: LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
John O’Connor and McKnight’s: A 36-year run
like no other
-
‘Confounding and heartbreaking’: Provider
groups decry Supreme Court decision that could see the departure of
immigrant workers
-
National Health Expenditure Projections,
2025–34: Strong Utilization Growth Initially, Legislative Impacts Later
-
Testimony of Bill Hammond on Medicaid’s
Consumer Directed Personal Assistance Program
-
Protecting Patients and Taxpayers:
Combating Healthcare Fraud and Leakage to Strengthen Program Integrity
-
What Surprises Aging Guru Ken Dychtwald
-
Americans Fear Navigating Long-Term Care
Alone More Than Affording It
-
I quit my job to care for my sick husband.
A little-known program provided training and pays me to do it
-
Political Insights from the 2026 Social
Security and Medicare Trustees’ Reports
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Friday, June 26,
2026, 10:03 AM (Pacific)
Seattle—
#############################
LTC BULLET: LTC HOAX?
LTC Comment: The media and
researchers constantly misrepresent Medicaid LTC spend down. Is it a
genuine misunderstanding, a deliberate hoax, or something else? Answers
after the ***news.***
|
*** TODAY'S LTC BULLET is sponsored by Claude
Thau (BackNine Insurance). BackNine gives you a free
personalized website at no cost. Your clients (& family & friends)
can, with as little or as much of your involvement as you or they
want, buy life insurance and LTCi, and can speed issue by scheduling a
paramed and uploading medical records immediately. We quote
stand-alone LTCi, linked-benefit and life with a LTC rider
side-by-side. Claude is the lead author of Milliman’s annual Broker
World LTCi Survey & a past Chair of the Center for Long-Term Care
Financing. Contact him at 913-707-8863 or
claude@back9ins.com to learn about more
great BackNine features and services. *** |
*** CASE IN POINT: Here’s
the LTC Hoax in action. I penned the following letter to the editor of
Health Affairs about an article the journal published that gets
Medicaid LTC financial eligibility wrong. Of course, my letter wasn’t
published.
Here’s why.
Peer review is like a moat protecting the
LTC Narrative
that government is the solution to all LTC problems
Letter to the editor of
Health Affairs regarding “Medicaid Asset Limits And Enrollment
Among Older Adults And People With Disabilities” (https://doi.org/10.1377/hlthaff.2025.01437)
This article on Medicaid
asset limits displays a misunderstanding of Medicaid’s purpose and
operation in long-term care (LTC). Medicaid is not designed to promote
savings or minimize enrollment barriers; it is a safety net intended for
those who lack the means to pay for necessary care. To evaluate it through
the lens of enrollment friction obscures its core function.
The authors focus on
nominal asset limits, yet these limits are often circumvented in practice.
Applicants can convert countable assets into exempt forms—such as home
equity, personal property, or prepaid funeral expenses—allowing
individuals with substantial wealth to qualify. Similarly, income
eligibility rules permit high-income individuals to qualify once private
medical expenses are deducted. As a result, Medicaid LTC eligibility often
extends well beyond the truly needy.
The article’s empirical
findings—that some individuals who exceed asset thresholds are less likely
to enroll—are unsurprising and add little insight. More important is what
the analysis omits: how current rules enable middle- and upper-income
individuals to access publicly funded care while lower-income individuals
must spend down to near-total impoverishment before qualifying.
This dynamic has broader
consequences. More affluent individuals can access higher-quality
providers by paying privately before transitioning to Medicaid, while
providers must absorb lower reimbursement rates once that transition
occurs. This strains the care system and limits resources available for
the most vulnerable.
A more relevant line of
inquiry would examine why individuals with substantial assets can qualify
for Medicaid LTC at all, and how policy design might better align the
program with its intended role as a safety net for those most in need. ***
LTC BULLET: LTC HOAX?
I’ve wondered for years
how the actual results of Medicaid LTC spend down policy—easy access to
benefits while preserving wealth—can be so radically different from the
way they are presented in the media and scholarly publications, that is,
catastrophic spend down for care until total impoverishment. Do the
experts really not understand how Medicaid financial eligibility works? Or
do they know the truth but evade the reality because it doesn’t fit their
ideological proclivity toward government intervention? Perplexed, I
decided to enlist AI to help answer the question.
My Query to Gemini:
Medicaid financial
eligibility rules for long-term care (LTC) benefits allow people with high
incomes to qualify if their private medical or LTC expenses are
commensurately high because those private expenditures are deducted from
their income before the program's low income standard is applied.
Likewise, high asset people can qualify because most large assets seniors
own are exempt and countable assets are easily converted to exempt status
by simply using them to purchase non-countable resources. Unlike the
requirement for income spend down, that it be for documented private
health care expenses, however, there is no such requirement for asset
spend down. Asset spend down can be used to convert countable into
non-countable wealth in any amount. See “Medicaid’s
$100+ Billion Leak”
for details. Although this is true and indisputable, the conventional
wisdom repeated constantly in the media and often in scholarly sources is
that Medicaid LTC eligibility requires "impoverishment" and that people
all across America are spending down into destitution for LTC before they
qualify for Medicaid. Please give me a dozen or more examples of media or
academic sources that say Medicaid LTC eligibility requires
impoverishment. Then opine on why this mismatch between the reality and
the reporting persists decade after decade.
Gemini’s Answer:
You’ve identified a
significant gap between the technical reality of Medicaid planning and the
"impoverishment" narrative that dominates public discourse. Technically,
the "spend down" for assets does not require destitution in the way it is
often portrayed. Strategies like Medicaid Compliant Annuities, Caregiver
Agreements, and Equity-to-Exempt transfers allow for the preservation of
significant wealth. However, the media and academic framing consistently
emphasize a binary choice: pay out-of-pocket until broke, or qualify for
Medicaid only after reaching rock bottom.
Below are 12+ examples
of this narrative across mainstream media, advocacy groups, and academic
contexts.
Media & Journalism
These sources often
frame Medicaid LTC as a "safety net for the destitute," frequently
omitting the legal mechanisms used to protect assets.
- AP News
(2026): "Deliberately putting yourself or a relative into poverty so
Medicaid picks up the costs... Assistive living and nursing home care
often force families to exhaust their resources before qualifying." —
A Medicaid ‘spend down’ may get an older person LTC coverage.
- The New
York Times (2023): In various "Your Money" and "The New Old Age"
columns, the narrative often focuses on the "catastrophic" cost of care
that "drains life savings" to reach the $2,000 asset limit. Has referred
to the "Catch-22" of Medicaid where seniors must "spend down until they
are virtually penniless."
- CNBC
(2024): Business reporting frequently highlights that Americans are
"forced to spend down into poverty" to access long-term care benefits.
- KFF
(Kaiser Family Foundation): While technically accurate on rules,
their public briefs often headline the "limited financial resources" and
"low-income" nature of beneficiaries as a prerequisite.
- The
Washington Post: Often features op-eds or "Health & Science"
features describing the "vicious cycle of spending down every last cent"
to qualify for nursing home coverage. Reports on families "spending down
to the bone" to meet the $2,000 asset limit.
- Forbes:
While some articles discuss "Medicaid planning," many general finance
columns warn that LTC requires you to "impoverish yourself" to let the
government take over.
- The Wall
Street Journal: Often describes the "cruel choice" of "emptying the
bank account" to qualify for government help with long-term care.
- NPR:
Features stories on the "exhausting process" of "becoming poor enough"
to get Medicaid coverage for a spouse.
- PBS
NewsHour: Has framed segments on long-term care around the idea that
Americans must "become destitute to get help."
- CNBC:
Articles on retirement planning frequently warn that "long-term care can
impoverish you" before Medicaid kicks in.
Advocacy & Public
Interest Groups
These organizations
often use the "impoverishment" language to argue for better funding or
policy changes.
- AARP:
Frequently publishes guides stating that to qualify for Medicaid, you
must have "very little in the way of assets," reinforcing the idea that
the program is only for the poor.
- Center
for Medicare Advocacy: Highlights that current rules result in the
"impoverishment of older people and people with disabilities" due to the
high cost of out-of-pocket care. Notes that without spousal protections,
many would be "left with, literally, no income at all" and that
residents are "in jeopardy" of destitution.
- American
Health Care Association (AHCA): Often refers to the Medicaid
population in nursing homes as "low-income seniors" or "vulnerable
residents" who have no other options.
- Justice
in Aging: Focuses on the "economic insecurity" of seniors, framing
the eligibility process as a transition into poverty.
- NCOA
(National Council on Aging): Explains that "you must spend down
into poverty" to qualify for the Medically Needy program in many
states.
Academic & Policy
Research
Even in scholarly work,
the "Spend Down = Destitution" model is often the baseline assumption for
policy simulation.
- Health
Affairs: Numerous articles over the decades use the term "Medicaid
Spend-Down" as a synonym for the depletion of wealth by middle-class
seniors. Frequently discusses the "risk of impoverishment" for those
needing long-term services and supports (LTSS), framing the lack of
social insurance as a path to "financial destitution."
- Journal
of the American Medical Directors Association (JAMDA): Recent
studies emphasize that facilities are serving "the most impoverished
communities," linking Medicaid status directly to lack of wealth.
- The
Gerontologist: Academic papers frequently explore the "psychological
toll of spend-down," describing the process as one where seniors must
"bankrupt themselves" to get care. Research papers often categorize the
"medically needy" as those who have reached a state of "functional
poverty" through medical expenses.
- Urban
Institute: Policy briefs often describe Medicaid as the program for
those who have "exhausted their private resources" through the high cost
of long-term services.
- ASPE (HHS):
"Asset spend-down in nursing homes is the process by which
individuals... deplete their available assets... and then enroll in the
Medicaid program once they are impoverished." — A Synthesis
and Critique of Studies on Medicaid Asset Spenddown.
- Milbank
Quarterly: "Elderly persons with functional impairments must
impoverish themselves by incurring large out-of-pocket expenditures
on nursing-home care before becoming eligible for Medicaid benefits." —
Long-term Care, Medicaid, and Impoverishment of the Elderly.
- Journal
of the American Geriatrics Society (JAGS): Uses the term
"Medicaid-induced impoverishment" to describe the transition of
middle-class seniors into the program.
- Center
for Retirement Research (Boston College): Often frames studies
around the "likelihood of impoverishment" for retirees facing nursing
home stays.
-
Georgetown University (LTC Financing Project): Policy briefs
frequently state that Medicaid acts as a "safety net for those who have
exhausted their resources."
Key Nuance: The
"Myth" vs. The Narrative
There is a
counter-academic movement—most notably led by Stephen A. Moses of
the Center for Long-Term Care Reform—who has published extensively on
"The Myth of Medicaid Spend-Down."
The Reality:
While the media highlights the $2,000 asset limit, they rarely mention
that a primary residence (up to ~$700k–$1M+ depending on the
state), a vehicle, and irrevocable burial trusts are exempt.
Additionally, "Income Spend Down" is actually a "Spend Through," where the
applicant uses their income to pay their share of cost, while the
government covers the rest—hardly "destitution" if the care is being
provided.
The Reality vs. The
Narrative
As you noted, the
"indisputable" reality includes several legal avenues that prevent literal
destitution, yet they are rarely the focus of general reporting:
|
The "Impoverishment"
Narrative |
The Technical Reality |
|
"You must be penniless." |
You can keep a primary residence
(up to ~$713k–$1.07m equity), one car, and personal belongings. |
|
"You must spend all money on
care." |
You can spend "countable" cash
on "exempt" assets (e.g., home repairs, prepaying funerals, buying a
better car). |
|
"The spouse is left with
nothing." |
Spousal Impoverishment Rules (CSRA)
allow the community spouse to keep up to ~$154,140 in assets (2024/25
levels). |
|
"High income disqualifies you." |
"Income caps" can often be
bypassed via Miller Trusts (Qualified Income Trusts) in many states. |
LTC Comment:
Follow up: based on your
findings, do you think this commonplace misrepresentation of the reality
is intentional to support an ideological bias or based only on ignorance?
AI:
The gap between the "impoverishment" narrative and the actual
mechanics of Medicaid eligibility isn't easily reduced to just a
malicious lie or just simple ignorance. Instead, it is a classic
example of structural bias—where institutional complexities, media
incentives, and political ideologies converge to create a distorted public
perception.
If you analyze the behavior of the groups
pushing this narrative, you can see a mix of well-meaning
oversimplification, strategic political positioning, and
commercial interest.
Here is how the motivations break down
across the spectrum:
1. The Media: The "Path
of Least Resistance" & Human Drama
For journalists, the misrepresentation is
driven less by a deep ideological conspiracy and more by occupational
constraints:
- Complexity: Medicaid is a
labyrinth of federal guidelines and 50 distinct sets of state rules.
Explaining "Medically Needy" income spend-down or the mechanics of a
Qualified Income Trust (Miller Trust) requires too many column inches
and bores the general reader.
- The "Unplanned" Reality: For the
vast majority of middle-class families who do not hire an elder
law attorney in advance, the experience feels like
impoverishment. They enter a crisis (e.g., a sudden stroke), go to a
nursing home, and are told they must pay $10,000/month out-of-pocket
until their liquid bank accounts hit $2,000. That is the story that
reaches reporters. The reporter writes about the crisis, missing the
fact that a proactive lawyer could have sheltered those assets.
- Narrative Arc: "Local senior
forced into poverty by broken healthcare system" is a compelling,
high-engagement headline. "Local senior successfully shifts wealth into
exempt asset categories using legal loopholes" is a technical financial
column.
2. Left-Leaning Academics
and Policy Advocates: Supporting Universal Care
For progressive think tanks and advocates,
framing Medicaid as requiring "impoverishment" serves a specific
ideological goal: the expansion of the social safety net.
- The Goal: They want a universal,
Medicare-for-all-style long-term care benefit.
- The Strategy: To build political
will for universal care, you must convince the middle class that they
too are at risk. If the middle class believes they can easily
navigate Medicaid rules to protect their inheritances, they won't vote
for expensive new government programs. By highlighting the $2,000 asset
limit and framing it as "destitution," they create pressure for systemic
reform.
3. Right-Leaning/Fiscal
Conservative Groups: Highlighting Welfare Abuse
Conversely, some conservative groups
actually agree with your premise—that Medicaid is easily
manipulated—but they use it to argue for stricter asset recovery and
tighter rules:
- They argue that middle-class or wealthy
seniors are "crowding out" the truly poor by hiding wealth in exempt
assets (like high-value homes or annuities).
- However, when these groups write
public-facing warnings, they often emphasize the "harshness" of the
rules to discourage people from relying on Medicaid, unintentionally
reinforcing the narrative that the program is punitive.
4. The Elder Law and
Long-Term Care Insurance Industries
There is a massive commercial incentive to
keep the "impoverishment" narrative alive:
- Long-Term Care Insurance (LTCI)
Companies: To sell a policy, they must terrify you. Their marketing
materials constantly declare: "A nursing home will wipe out your life
savings and leave you destitute!" They rarely mention that a good
attorney can shelter your assets without their insurance.
- Elder Law Attorneys: Ironically,
even though these lawyers specialize in proving Medicaid doesn't require
destitution, their marketing often leads with the threat of
impoverishment to get clients through the door: "Don't let the
nursing home take your house!"
Summary: Ignorance
Filtered Through Incentives
The Verdict: It is rarely pure,
conscious ignorance, but rather strategic framing.
Every player in the ecosystem has a reason
to emphasize the "scary" $2,000 cash limit rather than the "lenient"
exempt asset rules:
- Advocates want to show the
system is cruel so it will be changed.
- Journalists want a dramatic
story about human suffering.
- Businesses want to sell you a
product (insurance or legal services) to protect you from that cruelty.
The legal reality you pointed out—that a
senior can buy a $500,000 exempt home, buy a brand new car, pay off a
mortgage, and prepay funerals to qualify for Medicaid—is an open secret
among lawyers, but a deeply inconvenient truth for almost every major
narrative or commercial interest in the space.
Closing LTC Comment: Well, there
you have it. Misrepresenting Medicaid financial eligibility policy to
suggest it requires spend down into impoverishment is not a hoax
(deliberate deceit) according to AI, but only different groups pursuing
their self-interests. Smooth, I say. That lets everyone off the hook of
thinking about what would be better public policy. Maybe you can excuse
senior advocates and business enterprises for pursuing their narrow
interests. But should we exonerate Medicaid planners who manipulate the
rules to help affluent clients for big fees at the expense of the
genuinely needy? Should scholars who ought to pursue objective truth get a
pass? No, I think the term “LTC Hoax” applies accurately to them. They
allow a self-serving lie to take precedence over truthful analysis in
pursuit of better public policy.
To make sense of what ails LTC, read the
Paragon Health Institute’s “Long-Term
Care: The Problem” and “Long-Term
Care: The Solution” and watch this “virtual
LTC event” featuring age wave visionary Ken Dychtwald and leading LTC
researchers. To find ample private funds for LTC, check out “Medicaid’s
$100+ Billion Leak.” For what not to do, see “Medi-Cal-amity:
California’s Reckless Expansion of Medicaid Long-Term Care to the Affluent.”
See also “Better
Long-Term Care for Billions Less.” Find much more on long-term care
here.
#############################
Updated
Monday, June 22, 10:03 AM (Pacific)
Seattle—
#############################
LTC E-ALERT #26-021: LTC NEWS AND COMMENT
LTC Comment: Do you spend hours searching
the internet for useful articles, key data, and relevant reports to keep
you on the forefront of professional knowledge? Do you lose business
because you’re blindsided by clients or competitors who learn critical
information before you do? Here’s an antidote:
LTC Clippings: The Center for Long-Term
Care Reform notifies subscribers to our LTC Clippings service daily of
information you need to know. Each message contains only the critical
facts about new publications: a title, representative quote, a link to
the original, and our analysis in a sentence or two. To inquire or
subscribe, contact Damon at 206-283-7036 or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC E-Alerts: Once a week, we compile our
daily LTC Clippings into a summary, email it to Center for Long-Term Care
Reform members, and archive it in The Zone, our password-protected
members-only website. Center members also receive our weekly LTC Bullet
op-ed. To join the Center and receive all these benefits and more,
contact Damon at 206-283-7036 or
damon@centerltc.com.
We no longer post our LTC E-Alerts on the
Center’s public access website, but here’s what today’s LTC E-Alert
contained: links, quotes and comments on the following articles, reports,
or data:
-
What is Socialism?
-
‘Will I spend my 50s or 60s as a caregiver?’: A
woman in an age-gap relationship started doing 'grief math' — and it
exposed a financial blind spot
-
Senior living communities charging more for the
room, less for the care
-
5 Contentious Reasons the Middle Class Hasn't
Bought Long-Term Care Insurance
-
Social Security Is In Far Worse Shape Than We're
Being Told: The System's $71.9 Trillion Unfunded Liability Is Over Twice
What its ‘Trustees’ Mention
-
Spending on Medicaid State Directed Payments Before
New Limits Take Effect
-
Federal Medicaid Spending Through State Directed
Payments Nears $100 Billion Annually Across 41 States, With New Limits
Set to Reduce Funding to States
-
Senior living industry backs new CMS Medicaid
waiver oversight rules
#############################
"LTC E-Alerts" are
a
feature offered by the Center for Long-Term Care Reform, Inc. to members
at the $150 per year level or higher. We'll track and report to you news
and analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Monday, June 15, 10:03 AM
(Pacific)
Seattle—
#############################
LTC
E-ALERT #26-020: LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
A New Option for Long-Term Care Costs
-
Advisors Aren't Ready For The 30-Year
Retirement, Ken Dychtwald Argues
-
Medicare Advantage Organizations overturned
most SNF denials, OIG finds
-
The Nation's Fiscal Health: Urgent and
Sustained Action Needed to Improve the Fiscal Outlook
-
What’s in the 2026 Medicare Trustees
Report?
-
Social Security funds could run short by
2032, program's Trustees warn
-
A Closer Look at the IRS LTC Guidance
-
What to Know About Recent Federal Actions
Involving State Medicaid Program Integrity
-
Ohio suspends 49 home health providers from
Medicaid program over fraud concerns
-
Long-term care reform plans spark
widespread backlash in Germany
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Friday, June 12, 2026, 10:03 AM (Pacific)
Seattle—
#############################
LTC BULLET: WHAT IS
MEDICAID FOR?
LTC Comment: These
scholars publishing in a peer-reviewed journal do not understand
Medicaid’s purpose, nor how it hurts the poor and helps the well-to-do. We
explain after the ***news.***
*** Share Your Working Caregiver Story
CareScout and Genworth, in partnership with Share
More Stories, are inviting working caregivers to participate in a
storytelling-based research project focused on the real experience of
balancing work and caregiving.
By sharing an audio or written story through the SEEQ
platform, caregivers can help deepen understanding of the emotional and
practical realities they face, and contribute to more effective support(s)
in the future.
Eligible participants receive a $25 gift card.
Learn more and participate:
https://sharemorestories.com/working-caregiver-experience-carescout-seeq/
***
LTC BULLET: WHAT IS
MEDICAID FOR?
LTC Comment: The
following article in the current issue of Health Affairs is a
confused mishmash of mistaken notions that never should have passed peer
review. The complete piece does not deserve your attention, but the
abstract is worth our brief scrutiny. It displays the confusion, common
among Medicaid LTC researchers, regarding the Medicaid program, its
legitimate purpose and how it diverges in practice from official
objectives. Here’s the article, its abstract, and our line-by-line review.
“Medicaid
Asset Limits and Enrollment Among Older Adults and People With
Disabilities,” by Andrew Anderson, Chau
Huynh, and Catherine K. Ettman, Health Affairs, 45, NO. 6 (2026):
708–715.
ABSTRACT Medicaid asset
limits determine how many countable resources older adults and people with
disabilities may retain while qualifying for coverage. Although intended
to target benefits to those with the greatest financial need, these rules
may discourage saving and create administrative barriers to enrollment.
Amid recent federal and state reforms to update asset limits and a new
federal home equity cap of $1 million taking effect in 2028, we examined
how many income-eligible older and disabled adults are affected by
Medicaid asset limits and whether exceeding these limits is associated
with lower enrollment. Using nationally representative data for 2023, we
estimated that among 6.2 million income-eligible adults not enrolled in
Medicaid, 1.5 million (24.7 percent) exceeded their state’s financial
asset limit and 387,525 (8.6 percent) exceeded the home equity limit.
Regression discontinuity models indicated that exceeding financial asset
thresholds was associated with lower enrollment among unmarried adults.
Asset limits thus exclude a modest share of otherwise-income eligible
people overall but may disproportionately burden subgroups with limited
financial resources.
LTC Comment:
Let’s dissect this abstract sentence by sentence to see if we can make
sense of it, or at least explain what it gets wrong.
Abstract:
“Medicaid asset limits determine how many countable resources older adults
and people with disabilities may retain while qualifying for coverage.”
LTC Comment:
This is true and the limit on countable resources is usually very low,
often $2,000. But the official limit is irrelevant because there is no cap
on how much countable wealth applicants can convert to non-countable
status simply by purchasing exempt assets. Pay off a mortgage or add a
room to increase home equity, buy a nicer car, prepay funeral expenses,
purchase expensive new personal and household belongings, acquire a
business or rental property, and so on. There is practically no limit to
how much wealth the affluent can shelter and retain in this way. See “Medicaid’s
$100+ Billion Leak for details.”
Abstract:
“Although intended to target benefits to those with the greatest financial
need, these rules may discourage saving and create administrative barriers
to enrollment.”
LTC Comment:
What a peculiar notion. The purpose of Medicaid is not to encourage
savings or avoid administrative barriers to enrollment. It is to provide a
financially viable safety net of LTC services for people who have failed
to save and have become a financial and administrative burden on the
state. Medicaid should target benefits to those most in need and exclude
others of lesser or no need. These authors have Medicaid’s role upside
down and backwards.
Abstract:
“Amid recent federal and state reforms to update asset limits and a new
federal home equity cap of $1 million taking effect in 2028, we examined
how many income-eligible older and disabled adults are affected by
Medicaid asset limits and whether exceeding these limits is associated
with lower enrollment.”
LTC Comment:
What kind of question is that? If exceeding asset limits is not associated
with lower enrollment, something is obviously wrong. Otherwise, why set
limits on assets in the first place? Regarding the million dollar home
equity limit, it prevents very few people from qualifying for Medicaid LTC
benefits because the median home equity of elderly Americans,
$250,000, is only one-fourth of that
amount. A better research question would be: how many people with home
equity approaching a million dollars receive welfare-financed Medicaid
benefits and why is that allowed?
Abstract:
“Using nationally representative data for 2023, we estimated that among
6.2 million income-eligible adults not enrolled in Medicaid, 1.5 million
(24.7 percent) exceeded their state’s financial asset limit and 387,525
(8.6 percent) exceeded the home equity limit.”
LTC Comment:
Yes, and so, what’s their point? Affluent people don’t qualify for
Medicaid LTC benefits? If it were only that simple! These authors do not
understand how Medicaid LTC eligibility works in the real world. Forget
the low income and asset caps. What really happens is that income can be
very high because private health expenses are deducted before the low cap
is applied. Consequently, someone with $10,000 a month of income who has a
nursing home bill of comparable size is eligible based on income. Nor are
their assets actually limited because countable wealth is easily converted
to exempt resources as explained above.
Abstract:
“Regression discontinuity models indicated that exceeding financial asset
thresholds was associated with lower enrollment among unmarried adults.”
LTC Comment:
Do they really need fancy econometric models to discover that capping
income and assets excludes some people from eligibility? The resulting
inequity is much worse than these authors grasp as explained below.
Abstract:
“Asset limits thus exclude a modest share of otherwise-income eligible
people overall but may disproportionately burden subgroups with limited
financial resources.”
LTC Comment:
Well, yes, of course. And who do you think are the subgroups with limited
financial resources who are excluded? Answer. The poor, whom Medicaid was
supposed to help first. Private nursing home or home health expenses
quickly consume the limited resources of financially vulnerable people
leaving them totally impoverished. The middle class and affluent, on the
other hand, who should not rely on public welfare, are able to qualify for
Medicaid LTC benefits using the methods just described and others, such as
irrevocable income-only trusts. Even worse, these more financially able
people co-opt the best care Medicaid offers because they can afford to pay
privately for a time before they switch to Medicaid. That is because the
best nursing homes and home health agencies compete for private residents
who pay 150% of the Medicaid rate on average. After the financially
comfortable make the switch to Medicaid, state and federal laws prohibit
their being discharged simply because their source of payment changes. LTC
providers get stuck with the new low-revenue from formally private-pay
Medicaid recipients. This inhibits their ability to pay caregivers
adequately and to provide quality care.
Closing LTC Comment:
Is it clear now what is really going on? Instead of a safety net for the
poor, Medicaid forces the most vulnerable, least financially solvent
people to impoverish themselves. But the middle class and affluent not
only qualify quickly but they get the best care available through
Medicaid. Worse yet, instead of paying privately at market rates for their
care, which would contribute desperately needed revenue to the service
delivery system, these previously private-pay residents generate only 70%
of the private pay rate as Medicaid recipients. On top of everything, this
system effectively desensitizes most Americans to LTC risk and cost
leaving them uninsured and dependent on public assistance when their need
arises. How different this reality is from the confused Health Affairs
hodgepodge!
#############################
Updated Monday, June 8, 10:03 AM
(Pacific)
Seattle—
#############################
LTC
E-ALERT #26-019: LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
What This Year's Biggest Medicare Changes Mean for
You
-
Poverty and Dependency in the United States,
1939–2023
-
End-of-life costs at least 50 percent higher for
adults younger than 65, study finds
-
DHS: Only 2,000 of 5,600 high-risk Medicaid
providers revalidated upon review
-
How to Help Regular Clients Handle Long-Term Care
Costs
-
Immigration bans expected to lead to healthcare
workforce shortages, researchers say
-
Why 1035 Exchanges Are Becoming a Bigger Part of
LTC Planning Conversations
-
We couldn't afford to pay for my mom's dementia
assisted living anymore. She moved into a tiny house next door to me
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Monday, June 1, 10:03 AM
(Pacific)
Seattle—
#############################
LTC
E-ALERT #26-018: LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Sticker Shock In Seattle Over WA Cares' $36,500
Lifeline
-
IRS Guidance Shines Light on Post-SECURE 2.0
Long-Term Care Distributions
-
The growing long-term care dilemma
-
Senior living and care increasingly bifurcated,
with no room for the middle, experts say
-
Key Facts About Health Care Affordability for
People With Medicare
-
Proposed legislation signals broader trends senior
living providers should be watching, experts say
-
Annuities May Help Clients Live Longer: Study
-
Senators call for new Medicare benefit for home
care, more Medicaid HCBS funding
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Friday, May 29, 2026, 10:03 AM (Pacific)
Seattle—
#############################
LTC BULLET: AN OPEN
INVITATION TO LTC FRAUD
LTC Comment:
Government’s good intentions opened the flood gates for LTC fraud. We
explain after the ***news.***
|
*** TODAY'S LTC BULLET is sponsored by Claude
Thau (BackNine Insurance). BackNine gives you a free
personalized website at no cost. Your clients (& family & friends)
can, with as little or as much of your involvement as you or they
want, buy life insurance and LTCi, and can speed issue by scheduling a
paramed and uploading medical records immediately. We quote
stand-alone LTCi, linked-benefit and life with a LTC rider
side-by-side. Claude is the lead author of Milliman’s annual Broker
World LTCi Survey & a past Chair of the Center for Long-Term Care
Financing. Contact him at 913-707-8863 or
claude@back9ins.com to learn about more
great BackNine features and services. *** |
*** LTC CLIPPINGS notify
Center premium members of news and analysis in real time. Steve Moses
scans the media and academic journals; he picks the most important news
and analysis to keep you at the professional forefront; and he gives you
the source, a representative quote, and his brief analysis. A couple
examples follow. Find our “Membership Levels and Benefits Schedule”
here. Join the Center and become a
premium member
here. Or contact
damon@centerltc.com for details.
5/27/2026,
“Key
Facts About Health Care Affordability for People With Medicare,”
by Nancy Ochieng, Meredith Freed, Juliette Cubanski, Jeannie Fuglesten
Biniek, and Tricia Neuman, KFF
Quote:
“Long-term services and supports, which are not covered by Medicare, are
unaffordable for all but the highest-income Medicare beneficiaries. In
2025, the median
annual costs of common long-term
services and supports in the U.S were
$80,080 for full-time non-medical caregiver services (including home
health aide and homemaker services for people who need help with
instrumental activities of daily living such as preparing meals and doing
laundry), $129,575 for a private room in a nursing home, and $305,760 for
round-the-clock home health aide services (Figure 9). These costs greatly
surpass median income ($43,200)
and savings ($110,100) among people with Medicare. Long-term care services
are generally not covered by Medicare, regardless of whether a beneficiary
is enrolled in traditional Medicare or Medicare Advantage.”
LTC Comment:
Every few years, KFF publishes a version of this message saying that
Medicare beneficiaries are too poor to afford LTC. You’re supposed to
conclude that LTC costs devastate people on Medicare who need extended
care that Medicare does not cover. The truth is that Medicaid pays the
catastrophic LTC costs of Medicare beneficiaries who have the need. We
explained how this works in two LTC Bullets:
Hoist with its Own Petard and
KFF Hoisted Again. Read them for relief
from KFF’s dystopian views and for ideas on how to fix LTC financing
without adding it to Medicare.
5/26/2026,
“Senators
call for new Medicare benefit for home care, more Medicaid HCBS funding,”
by John Roszkowski, McKnights Home Care
Quote:
“A group of Democratic United States senators last week expressed the need
for a new Medicare benefit for in-home care and expanded Medicaid funding
for home- and community-based services as part of a larger plan to
increase funding for long-term care services.”
LTC Comment:
First, float the Titanic (Medicare) before adding more deck chairs (LTC
benefits). ***
LTC BULLET: AN OPEN INVITATION TO LTC FRAUD
LTC Comment: Health care
fraud is all
over the news lately. Medicaid and
Medicare are the fraudsters’ favorite targets. Medicaid LTC is especially
vulnerable because most of it (87.1% at latest count) is provided in
unsupervised home and community-based settings. That makes billing for
undelivered services and other fraudulent measures tempting, easy and hard
to catch.
The Centers for Medicare
and Medicaid Services (CMS) is fighting a rearguard action to rein in
health care fraud. The Administration’s
Comprehensive Regulations to Uncover Suspicious Healthcare
(CRUSH) initiative and a
Task Force to Eliminate Fraud aim to
curtail fraud in CMS programs estimated to cost
$100 billion per year. Some say these
measures are
too little, too late. Why hasn’t the
government fought fraud more aggressively up to now?
Efforts to fight fraud
in public benefit programs face many obstacles. The huge volume of
transactions; legal limits on the government’s ability to exclude
questionable providers, and sluggish public sector implementation of
technological advances, all impede progress against fraud. Third parties,
especially Medicaid and Medicare, fund most health care, including LTC,
which creates a
moral hazard that invites fraud. The
gigantic size of government health care programs and the fragmentation
between programs and between federal and state-level funding and
administration of Medicaid impair fraud identification and control.
All these factors
contribute, but the biggest obstacle to public sector fraud control comes
from legal constraints. Medicaid and Medicare were created in 1965 as part
of Lyndon Johnson’s Great Society war on poverty. The new programs
entitled people to a wide range of medical and LTC services. After
enactment, their costs exploded immediately. State and federal efforts to
control costs led to litigation aimed at protecting the public’s access to
the new entitlements. Two major court cases addressed this issue.
In
Goldberg v. Kelly [1970], the Supreme
Court ruled that before the government can terminate an individual’s
statutory entitlement like welfare or health benefits, it must provide a
pre-termination hearing. This means if the government suspects fraudulent
billing or ineligibility in Medicaid, it cannot simply stop payments
immediately. It must give the recipient notice and an opportunity to be
heard, making swift fraud intervention administratively burdensome.
Consequently, nearly all government fraud control must be done using a
“pay and chase” approach as opposed to preventing fraudulent payments
before they occur.
A second court case
moderated Goldberg’s highly constrictive decision. In
Mathews v. Eldridge, [1976] the Court set
a balancing test that agencies use to determine if a pre-termination
hearing is mandatory. It requires reviewing: (1) the individual's private
interest in uninterrupted benefits, (2) the risk of erroneous deprivation,
and (3) the government's interest, including fiscal and administrative
burdens. Thus, Mathews allowed the termination of Social Security
Disability benefits without a prior hearing. The Court reasoned that
disability determinations rely on objective medical evidence (unlike the
subjective, need-based criteria in Goldberg). Disabled workers were
deemed less likely to face immediate, life-threatening destitution than
welfare recipients, making retroactive post-termination payments an
acceptable remedy if the government is proven wrong.
These precedents show
that fighting fraud is not a simple cut-and-dry process for the
government. Because Medicaid and Medicare provide life-saving health care
and are treated as protected property rights, the government faces strict
constitutional (due process) constraints on how it halts patient benefits
or revokes provider billing privileges. Agencies must establish extensive,
time-consuming administrative protocols to minimize the risk of wrongly
targeting innocent recipients, which slows down their ability to stop
illegitimate payments.
Modern agencies struggle
to maintain accurate decision-making while dealing with millions of
claims. The tension between providing "court-like" procedures and managing
immense administrative systems frequently pushes federal programs into an
operational crisis. Administrative safeguards have created a decade-long
appeals backlog. This delay causes immense economic pressure on care
providers, even though many are eventually cleared of wrongdoing.
Constitutional due process requirements directly collide with available
agency funding, IT systems, and personnel.
There is a tension
between the Goldberg requirement for extensive pre-termination
hearings and the practical need for Medicaid Fraud Control Units (MFCUs)
to make immediate, summary suspensions to halt fraudulent billing.
The mandatory continuation of HCBS benefits pending an administrative
appeal allows unscrupulous providers and ineligible beneficiaries to
continue receiving funds, draining agency resources while lengthy fraud
investigations conclude. Goldberg v. Kelly’s strict pre-termination
hearing requirements—paired with the Eldridge balancing test—impair
state efforts to combat fraud, overbilling, and abuse in Home and
Community-Based Services (HCBS) programs.
Bottom line, what began
as the government’s intention to help people obtain health and long-term
care has deteriorated into an open invitation for criminals to profit from
the public largesse. This outcome is only one example of a larger problem.
When government replaces personal responsibility and initiative with a
legally enforceable right to publicly funded benefits, all kinds of
negative consequences occur. People thus “protected” are less likely to
recognize, evaluate and prepare privately for life’s many risks. This
leaves them dependent on and vulnerable to whatever promises government
has made. The sad irony is that after decades of the U.S. government
promising Social Security, Medicare and Medicaid, the American public is
unprotected today against the increasingly likely retrenchment of those
programs. When that happens, the unenforceable assurances from court cases
like
Goldberg v. Kelly and
Mathews v. Eldridge will be cold comfort.
#############################
Updated
Tuesday, May 26, 10:03 AM (Pacific)
Seattle—
#############################
LTC E-ALERT #26-017: LTC NEWS AND COMMENT
LTC Comment: Do you spend hours searching
the internet for useful articles, key data, and relevant reports to keep
you on the forefront of professional knowledge? Do you lose business
because you’re blindsided by clients or competitors who learn critical
information before you do? Here’s an antidote:
LTC Clippings: The Center for Long-Term
Care Reform notifies subscribers to our LTC Clippings service daily of
information you need to know. Each message contains only the critical
facts about new publications: a title, representative quote, a link to
the original, and our analysis in a sentence or two. To inquire or
subscribe, contact Damon at 206-283-7036 or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC E-Alerts: Once a week, we compile our
daily LTC Clippings into a summary, email it to Center for Long-Term Care
Reform members, and archive it in The Zone, our password-protected
members-only website. Center members also receive our weekly LTC Bullet
op-ed. To join the Center and receive all these benefits and more,
contact Damon at 206-283-7036 or
damon@centerltc.com.
We no longer post our LTC E-Alerts on the
Center’s public access website, but here’s what today’s LTC E-Alert
contained: links, quotes and comments on the following articles, reports,
or data:
-
9 million older adults are missing out on $58
billion in help with food, medicine, daily costs
-
Reed: Can these assets be saved?
-
Guaranteed income streams better predictor of
retirement stability than assets
-
Senate Democrats Vow To Develop A Long-Term Care
Reform Plan
-
Policyholders Who Sold Their Life Insurance
Received Nearly 9x More Than Insurers Offered In 2025
-
IRS Starts to Implement a Long-Term Care Insurance
Tax Incentive
-
Call for public consultation on Global Standards
for Long-Term Care
-
Fixing long-term care coverage
-
Long-Term Care Claimant Was Working Full Time in
Demolition, Transamerica Says
#############################
"LTC E-Alerts" are
a
feature offered by the Center for Long-Term Care Reform, Inc. to members
at the $150 per year level or higher. We'll track and report to you news
and analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Monday, May 18, 10:03 AM
(Pacific)
Seattle—
#############################
LTC
E-ALERT #26-016: LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
AARP report says state of assisted living sector is
‘cause for concern,’ but industry says it helps residents ‘live well’
-
My dad's dementia care costs $9,000 a month. I'm
selling my parents' home to pay for it
-
White House cuts $1.3 billion in Medicaid payments
to California
-
Medicare’s 6-month enrollment freeze on home health
and hospice: What senior living providers need to know
-
Genworth's CareScout Unit Gets a Line in the
Financial Report
-
Eighth Circuit hands Unum a clean win on
long-term-care denial
-
[Updated] CMS issues six-month moratorium on new
hospices, home health agencies nationwide
-
Housing costs affect older adults’ ability to pay
for assisted living, and here’s where costs hit hardest
-
State Reverses Managed Medicaid for Nursing Homes
After $91M Cost Spike in First Year
-
New ‘economic architecture’ needed for aging
population, report says
-
Financial Shocks, Caregiving Gaps and Inflation
Pressures Persist For Retirees
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Friday, May 15, 2026, 10:03 AM (Pacific)
Seattle—
#############################
LTC BULLET: PROTECTING
WHAT MATTERS
LTC Comment: Today’s
LTC Bullet is a shout out to LTC insurance maven and radio-talk-show
host Barry Fisher along with a link to our latest online conversation,
after the ***news.***
*** CRUSH
FRAUD—Dominating the LTC financing news this week is the federal
government’s growing effort to identify, discourage and prosecute health
care fraud. Medicaid-funded home care services are especially susceptible
to fraud because of the inherent difficulty of measuring and monitoring
them. LTC Clippings recently highlighted some of the fraud news.
Examples follow. If you don’t have a subscription to LTC Clippings,
contact
damon@centerltc.com or call 206-283-7036.
Premium Center members receive all Center publications including the
bi-weekly LTC Bullets, weekly LTC E-Alerts, and daily LTC
Clippings. For all membership options, check out the Center’s “Membership
Levels and Benefits Schedule.”
5/13/2026,
“White
House cuts $1.3 billion in Medicaid payments to California,”
by Robert King, Politico
Quote:
“The Trump administration is withholding $1.3 billion in Medicaid
reimbursements to California for failing to combat fraud, escalating a
feud with the state over its management of hospice care. … Though the
administration has repeatedly criticized California’s fraud oversight,
this is the first time the Centers for Medicare and Medicaid Services has
targeted payments to the state.”
LTC Comment:
Do you think that’s excessive? Is it more important to support services
freely than to be vigilant about fraud? That’s the attitude of
some who criticize the current crackdown.
Before you buy into the “be happy, don’t worry” dialogue, go to
Paragon Health Institute, search for
“California,” and read the papers that pop up. Check out Paragon’s
Health Care Fraud Dashboard. And don’t
miss Paragon president Brian Blase’s
interview of Dr. Mehmet Oz, Administrator
of CMS.
5/14/2026,
“Medicare’s
6-month enrollment freeze on home health and hospice: What senior living
providers need to know,” by Kimberley
Bonvissuto, McKnights Senior Living
Quote:
“A six-month, federal moratoria on new Medicare enrollment for home health
and hospice agencies has the potential to affect a growing percentage of
senior living residents, but the action has the support of senior living
industry advocacy groups, provided the stoppage achieves the government’s
intended goal of allowing legitimate providers to deliver quality
services. The Centers for Medicare & Medicaid Services announced the
moratoria on Wednesday, effective immediately, in an effort to ‘protect
Medicare beneficiaries and taxpayer dollars.’ The move will enable CMS to
temporarily halt the influx of new providers into what it calls ‘high-risk
categories’ for fraudulent activity.”
LTC Comment:
CMS shuts down new home health and hospice activity and the industry is in
favor? Sounds counterintuitive until you consider that companies currently
in the business are protected from new competition entering the field. It
reminds me of the impact of certificate of need laws, intended to control
costs, that had the actual effect of protecting the nursing home industry
from competition. Let’s hope the current moratoria have the intended
effect of keeping new bad actors out of the business without unfairly
benefiting current companies. ***
LTC BULLET: PROTECTING
WHAT MATTERS
LTC Comment: Barry
Fisher, of
Blaze ‘n Bear Insurance Services, Inc.,
is a longtime friend and fellow fighter to improve long-term care. Barry’s
insurance career spans more than four decades working in the field of
personal financial well-being and responsibility. During most of that time
he has generously provided both financial and moral support for our work
at the
Center for LTC Reform. With broad
expertise in life, disability and long-term care insurance he works with
individuals, business owners and allied professionals helping them provide
protection for themselves and those they care about. Barry’s long and
distinguished career prepared him uniquely to create and host a radio talk
show he named “Protecting What Matters.”
“Protecting What
Matters” is “the broadcast that helps you become better informed about
services and products to protect various aspects of your life and
property.” Topics covered are wide-ranging, but all hew to the theme of
helping listeners become better, more successful consumers. Show subject
matter examples include: life, disability and long-term care planning and
insurance; commercial and personal property and casualty insurance;
personal finance and investment; business valuation; commercial and
residential lending; property rights; personal and spiritual growth; pets
and animal husbandry; physical, emotional and intellectual well-being;
economics; history; energy policy; taxes and legal matters; relationships;
“And whatever strikes our fancy!”
Of course, a recurring
theme in “Protecting What Matters” is long-term care financing, Medicaid,
Medicare, and the perverse public policies that have made such a mess of
that critical field. Barry brought me on to discuss LTC financing for the
third time on his Tuesday, May 12, 2026 show. You can hear what we had to
say
here. Just scroll down until you see the
Audio Player. Our section on LTC begins at 27 minutes, 24 seconds into the
program.
You can enjoy past shows
of Protecting
What Matters on the show’s dedicated
website and tune in Tuesdays at 1pm
Pacific Time on KPRL 1230 AM 99.3FM or listen to the live feed
here.
#############################
Updated
Monday, May 11, 10:03 AM (Pacific)
Seattle—
#############################
LTC E-ALERT #26-015: LTC NEWS AND COMMENT
LTC Comment: Do you spend hours searching
the internet for useful articles, key data, and relevant reports to keep
you on the forefront of professional knowledge? Do you lose business
because you’re blindsided by clients or competitors who learn critical
information before you do? Here’s an antidote:
LTC Clippings: The Center for Long-Term
Care Reform notifies subscribers to our LTC Clippings service daily of
information you need to know. Each message contains only the critical
facts about new publications: a title, representative quote, a link to
the original, and our analysis in a sentence or two. To inquire or
subscribe, contact Damon at 206-283-7036 or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC E-Alerts: Once a week, we compile our
daily LTC Clippings into a summary, email it to Center for Long-Term Care
Reform members, and archive it in The Zone, our password-protected
members-only website. Center members also receive our weekly LTC Bullet
op-ed. To join the Center and receive all these benefits and more,
contact Damon at 206-283-7036 or
damon@centerltc.com.
We no longer post our LTC E-Alerts on the
Center’s public access website, but here’s what today’s LTC E-Alert
contained: links, quotes and comments on the following articles, reports,
or data:
-
New ASHA
publication helps industry disprove senior living, home care
misconceptions
-
My Beloved Husband
Has Early-Stage Dementia. He Is 'Doing Well,' but How Do I Protect Our
$1.6 Million Savings Right Now?
-
Rural residents
less likely to receive HCBS than urban counterparts, study finds
-
Long-Term Care
Costs Are Hollowing Out Generational Wealth
-
Majority Of
Americans At Risk Of Outliving Their Retirement Savings
-
Study: Poor
housing affordability associated with higher risks of frailty, mortality
-
Medicaid
self-directed care has a fraud problem, Addus CEO says
-
What To Do About
Medicaid’s Long-Term Care Benefit?
-
Family caregiving
inflicts emotional, financial toll, new US News survey finds
-
The Old Guard
#############################
"LTC E-Alerts" are
a
feature offered by the Center for Long-Term Care Reform, Inc. to members
at the $150 per year level or higher. We'll track and report to you news
and analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Monday, May 4, 10:03 AM (Pacific)
Seattle—
#############################
LTC E-ALERT #26-014: LTC NEWS AND COMMENT
LTC Comment: Do you spend hours searching
the internet for useful articles, key data, and relevant reports to keep
you on the forefront of professional knowledge? Do you lose business
because you’re blindsided by clients or competitors who learn critical
information before you do? Here’s an antidote:
LTC Clippings: The Center for Long-Term
Care Reform notifies subscribers to our LTC Clippings service daily of
information you need to know. Each message contains only the critical
facts about new publications: a title, representative quote, a link to
the original, and our analysis in a sentence or two. To inquire or
subscribe, contact Damon at 206-283-7036 or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC E-Alerts: Once a week, we compile our
daily LTC Clippings into a summary, email it to Center for Long-Term Care
Reform members, and archive it in The Zone, our password-protected
members-only website. Center members also receive our weekly LTC Bullet
op-ed. To join the Center and receive all these benefits and more,
contact Damon at 206-283-7036 or
damon@centerltc.com.
We no longer post our LTC E-Alerts on the
Center’s public access website, but here’s what today’s LTC E-Alert
contained: links, quotes and comments on the following articles, reports,
or data:
-
At the Tipping Point: Liberating a New Age of Aging
-
New Law Caps Home Equity for Medicaid Long-Term
Care
-
Alzheimer’s deaths have more than doubled between
2000 and 2024, new report finds
-
The Association of Medicaid Estate Recovery with
Homeownership, Home Equity, and Medicaid Enrollment
-
Kennedy’s recent comments on paid family caregivers
‘deeply concerning,’ advocates say
-
Medicaid Waste, Fraud, and Abuse: Why CMS’s
Improper Payment Rate Can’t Be Trusted
-
BREAKING NEWS: CMS issues updated 2026 spousal
impoverishment standards
-
The longevity revolution is here. Our systems still
think we die at 65
#############################
"LTC E-Alerts" are
a
feature offered by the Center for Long-Term Care Reform, Inc. to members
at the $150 per year level or higher. We'll track and report to you news
and analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Friday, May 1, 2026, 10:03 AM (Pacific)
Seattle—
#############################
LTC BULLET: BRIDGING LTC
SILOS
LTC Comment: LTC providers and insurers
communicate too little, hewing jealously to their professional bailiwicks.
We try to narrow the gap after the ***news.***
*** LTC CLIPPINGS:
Did you catch these stories this week? Our LTC Clippings
subscribers received them in real time including Steve Moses’s always
trenchant, often ironic, sometimes humorous, usually concise “LTC
Comments.” To subscribe or for a free trial, contact Damon at
206-283-7036 or
damon@centerltc.com. Examples below:
4/28/2026, “New
Law Caps Home Equity for Medicaid Long-Term Care,” by Lee Pruitt,
ElderLawAnswers
Quote: “A new federal law,
effective in 2028, will cap the amount of home equity a person can have
and still qualify for Medicaid long-term care at $1 million. This $1
million limit will not increase with inflation, meaning more homeowners
will be affected over time as property values rise. If your home equity is
near or above $1 million, consult an elder law attorney now to explore
options like reverse mortgages or legal transfers before the 2028
deadline.”
LTC Comment: Good advertising hook
for Medicaid planners, huh? An open invitation to ignore private LTC
insurance and rely on taxpayers to protect home equity from LTC risk.
What’s even worse, the same Medicaid planners will tell people with less
home equity and a lot of cash to convert the countable cash to exempt
status by added spending on the home. After they pay the attorney’s fee
first, which is also exempt. Just another example of “What’s
Worse than Medicaid Fraud.”
----------------------
4/27/2026,
“Medicaid
Waste, Fraud, and Abuse: Why CMS’s Improper Payment Rate Can’t Be Trusted,”
by Chris Medrano and Brian Blase, Paragon Health Institute
Quote:
“Medicaid’s improper payment rate is widely misunderstood. PERM provides a
narrow compliance estimate and is not a reliable measure of waste, fraud,
abuse, or total improper payments in Medicaid. Major gaps in eligibility
determinations and managed care payments make PERM incomplete. The program
does not fully capture eligibility errors and fails to examine managed
care payments at the provider level—despite
managed care representing the majority of Medicaid spending. Low reported
error rates risk creating a false sense of security. Because PERM relies
on limited samples and lagged data, its findings understate risks and the
scale of improper payments. Policymakers should strengthen PERM to improve
accountability and enable enforcement actions in Medicaid.”
LTC Comment:
Bottom line: no one knows how much fraud, waste and abuse permeate
Medicaid because such limited measurements as exist are fatally flawed.
How refreshing that this critical subject is finally getting the attention
it deserves. ***
LTC BULLET: BRIDGING LTC SILOS
LTC Comment: Have you noticed how little the
people and companies responsible for providing long-term care (LTC)
communicate with the people and companies responsible for funding LTC?
You would think these two industries should have much to discuss. Nursing
homes and home health agencies desperately need revenue. LTC insurers
struggle to attract buyers. But the two professions rarely work together.
Both face a common problem. Medicaid pays LTC
providers too little, often less than the cost of providing the care. Easy
access to Medicaid when care is needed crowds out demand for private LTC
insurance. Logically, LTC providers and insurers would unite and mobilize
to advocate for policies that target Medicaid benefits to the neediest
Americans and divert the well-to-do toward private financing, so that they
pay economically sustainable market rates.
The Center for Long-Term Care Reform has
published
dozens of national and state-level studies
proposing policy solutions along those lines. Most recently, “Long-Term
Care: The Problem” and “Long-Term
Care: The Solution” with the
Paragon Health Institute. At the same
time, we have placed articles and columns in trade journals and other
publications intended to link the interests of LTC providers and insurers.
Following are some examples from October 2021 through April 2024. We hope
you’ll open and read some of them and that they will help tie together the
interests and policies of LTC providers and insurers.
- “The
Medicaid LTC snafu,”
by Stephen A. Moses, McKnights LTC News, April 15, 2024 (PDF
version.) This
article shows how Medicaid’s generous eligibility rules allow people
with significant income and assets to use Medicaid’s scarce resources.
- “Setting
the Record Straight on Long-Term Care Policy,”
by Stephen A. Moses and Brian Blase, Townhall, April 14, 2024 (PDF
version.) This
article debunks the claim, presented in The New York Times’
recent series Dying
Broke, that
catastrophic long-term care expenses are wiping out the savings of
American middle-class families.
- “How
government prevaricates about long-term care,”
by Stephen A. Moses, McKnights LTC News, February 23, 2024 (PDF
version.) This
article explores the biases in how federal officials and the media
report long-term care expenditures. It deconstructs the conventional
wisdom about out-of-pocket spending data.
- “Government
must encourage personal responsibility, prohibit easy access to Medicaid,”
by Steve Moses and Brian Blase, Washington Times, November 30,
2023. (PDF
version.) Save
Medicaid LTC for the needy by engaging self-interest and personal
responsibility.
- “The
federal Medicaid bait and switch,”
by Stephen A. Moses, McKnight’s LTC News, November 6, 2023. (PDF
version.) Medicaid
promised LTC providers generous revenue but reneged creating shortfalls
that hurt providers and consumers.
- "What’s
Wrong With Long-Term Care?,"
by Stephen A. Moses, RealClear Policy, November 2, 2022. (PDF
version.) This
article is a succinct explanation of what’s wrong with our long-term
care system and how to fix it.
- “LTC
insurance sales suddenly surge,”
by Stephen A. Moses, McKnight’s LTC News, August 10, 2022. (PDF
version.) It took
Washington State’s public long-term care insurance program to excite
private LTC insurance demand in that state to unbelievable levels. This
article explores this curious phenomenon and its important public policy
implications.
- “Long-term
care’s mortal risk,”
by Stephen A. Moses, McKnight’s LTC News, June 6, 2022. (PDF
version.) What if
our long-term care system collapses? This article explores how feeble
our long-term care system actually is.
- “Long-Term
Care Epiphany,” by
Stephen A. Moses, Broker World, June 2022. (PDF
version.) What if
the so-called “long-term care crisis” was really “no biggie”? This
article reconceptualizes the LTC conundrum and provides a solution.
- “Trappings
of LTC system leave operators trapped,”
by Stephen A. Moses, McKnight’s Long-Term Care News, February 23,
2022. (PDF
version.) This
article is a “thought experiment” exploring how a true free market can
vastly improve our long-term care system.
- “The
Great Long-Term Care Compromise,”
by Stephen A. Moses, Broker World, January 1, 2022. (PDF
version.) Using
Washington State’s WA Cares as a model, this article shows how to solve
the long-term care crisis by mandating people to choose between social
or private LTC insurance.
- “The
irony of long-term care advocacy,”
by Stephen A. Moses, McKnight’s Long-Term Care News, December 17,
2021. (PDF
version.) This
article examines the disconnect between the long-term care people want
and the long-term care public policy they get.
- “Long
Term Care Irony,”
by Stephen A. Moses, Broker World, December 1, 2021. (PDF
version.) When
forced to choose between public and private options for long-term care,
Washington State saw an unprecedented influx of private LTCi
applications. This article examines the historical context and primary
LTC myth driving such consumer behavior.
- “What
works for long-term care and what doesn’t,”
by Stephen A. Moses, McKnight’s LTC News, November 17, 2021. (PDF
version.)
This article gives a historical perspective of what’s gone wrong with
public financing of long-term care and how private financing can improve
it.
- “What’s
better for senior living and care — the market or government?,”
by Stephen A. Moses, McKnight’s Senior Living, October 25,
2021. (PDF
version.)
This article explains why and how markets succeed while government
usually fails.
#############################
Updated
Monday, April 27, 2026, 10:03 AM (Pacific)
Seattle—
#############################
LTC E-ALERT #26-013: LTC NEWS AND COMMENT
LTC Comment: Do you spend hours searching
the internet for useful articles, key data, and relevant reports to keep
you on the forefront of professional knowledge? Do you lose business
because you’re blindsided by clients or competitors who learn critical
information before you do? Here’s an antidote:
LTC Clippings: The Center for Long-Term
Care Reform notifies subscribers to our LTC Clippings service daily of
information you need to know. Each message contains only the critical
facts about new publications: a title, representative quote, a link to
the original, and our analysis in a sentence or two. To inquire or
subscribe, contact Damon at 206-283-7036 or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC E-Alerts: Once a week, we compile our
daily LTC Clippings into a summary, email it to Center for Long-Term Care
Reform members, and archive it in The Zone, our password-protected
members-only website. Center members also receive our weekly LTC Bullet
op-ed. To join the Center and receive all these benefits and more,
contact Damon at 206-283-7036 or
damon@centerltc.com.
We no longer post our LTC E-Alerts on the
Center’s public access website, but here’s what today’s LTC E-Alert
contained: links, quotes and comments on the following articles, reports,
or data:
-
CMS asks states to submit Medicaid provider
revalidation strategies, increase oversight
-
Medigap Premiums Leap, and Consumers Have Few
Alternatives
-
Dr. Oz announces a 50-state audit of Medicaid
program oversight
-
Exploring Early Uses of Artificial Intelligence in
Long-Term Care Systems
-
House hearing highlights ‘systemic failure’ at
heart of hospice, home health fraud
-
Americans Believe They Will Need $1.46 Million to
Retire Comfortably
-
Needing long-term care in retirement one of
Americans’ greatest fears, survey finds
-
State indicts 9 people on charges of fraud and
theft involving Medicaid
#############################
"LTC E-Alerts" are
a
feature offered by the Center for Long-Term Care Reform, Inc. to members
at the $150 per year level or higher. We'll track and report to you news
and analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Monday, April 20, 2026, 10:03 AM (Pacific)
Seattle—
#############################
LTC E-ALERT #26-012: LTC NEWS AND COMMENT
LTC Comment: Do you spend hours searching
the internet for useful articles, key data, and relevant reports to keep
you on the forefront of professional knowledge? Do you lose business
because you’re blindsided by clients or competitors who learn critical
information before you do? Here’s an antidote:
LTC Clippings: The Center for Long-Term
Care Reform notifies subscribers to our LTC Clippings service daily of
information you need to know. Each message contains only the critical
facts about new publications: a title, representative quote, a link to
the original, and our analysis in a sentence or two. To inquire or
subscribe, contact Damon at 206-283-7036 or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC E-Alerts: Once a week, we compile our
daily LTC Clippings into a summary, email it to Center for Long-Term Care
Reform members, and archive it in The Zone, our password-protected
members-only website. Center members also receive our weekly LTC Bullet
op-ed. To join the Center and receive all these benefits and more,
contact Damon at 206-283-7036 or
damon@centerltc.com.
We no longer post our LTC E-Alerts on the
Center’s public access website, but here’s what today’s LTC E-Alert
contained: links, quotes and comments on the following articles, reports,
or data:
-
What’s worse than
Medicaid fraud?
-
Henry Paulson Says
U.S. Should Prepare for a 'Vicious' Bond Crash
-
Alternative
Contingency Policies for When the Social Security Trust Fund Is
Exhausted
-
The Trump
Administration’s Anti-Waste in Health Care Campaign
-
$5,400 a Month for
Assisted Living Is the New Reality—How Families Are Making It Work
-
Report: Home
health providers ordered to pay over $100M in restitution for fraud in
2025
-
America Built No
System For Aging: The Largest Generation In History Just Started Turning
80
#############################
"LTC E-Alerts" are
a
feature offered by the Center for Long-Term Care Reform, Inc. to members
at the $150 per year level or higher. We'll track and report to you news
and analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Friday, April 17, 2026, 10:03
AM (Pacific)
Seattle—
#############################
LTC BULLET: LTC
INSURANCE FRAUD
LTC Comment: As
health insurance fraud surges nationwide, we consider how it impacts LTC
insurance in the private and public sectors after the ***news.***
*** LTC
CLIPPINGS: Did you catch these stories recently? Our LTC Clippings
subscribers received them in real time including Steve Moses’s
trenchant, often ironic, sometimes humorous, usually concise “LTC
Comments.” To subscribe or for a free trial, contact Damon at 206-283-7036
or
damon@centerltc.com. Examples below:
4/13/2026,
“Report:
With spend-down of assets, US long-term care system ‘effectively penalizes
aging’,” by Kathleen Steele Gaivin, McKnights Senior Living
Quote:
“Costs associated with the provision of long-term care in a system that
requires lower- and middle-class older adults to spend down their assets
to pay for home care or life in an assisted living community or skilled
nursing facility perpetuates ‘cycles of wealth inequality,’ making it
difficult for future generations to build financial security, according to
a new
study published by the Roosevelt Institute. … ‘This spend-down process
interrupts the potential for intergenerational wealth building, after what
is often a lifetime of work and saving by low-income and middle-class
families, perpetuating cycles of wealth inequality,’ Forden said.
‘Meanwhile, these costs are increasingly captured by profit-driven
corporations and private equity firms.’”
LTC Comment:
Medicaid asset spend down is the most misunderstood concept in LTC
financing jargon. It crushes the poor and lower middle class but gives the
middle-class and affluent an off ramp. Unlike income spend down that
requires spending for care, asset spend down can be done simply by using
countable wealth to purchase exempt resources. I explained how that works
and estimated how much it costs Medicaid (and taxpayers) in “Medicaid’s
$100+ Billion Leak.” Blaming “profit-driven corporations” for the
damage spend down does to those in need is just socialist claptrap. It’s
the “progressive” political proclivity to give everything to everyone and
print the money to pay for it that is the root of the problem. To make
sense of what ails LTC, read the
Paragon Health Institute’s “Long-Term
Care: The Problem” and “Long-Term
Care: The Solution” and watch this “virtual
LTC event” featuring age wave visionary Ken Dychtwald and leading LTC
researchers. To find ample private funds for LTC, check out “Medicaid’s
$100+ Billion Leak.” For what not to do, see “Medi-Cal-amity:
California’s Reckless Expansion of Medicaid Long-Term Care to the Affluent.”
Much more on long-term care
here. ***
4/16/2026, “Henry
Paulson Says U.S. Should Prepare for a 'Vicious' Bond Crash,” by
Christopher Amstey, Financial Advisor
Quote:
“Former Treasury Secretary Henry Paulson called on U.S. authorities to
prepare a back-up plan in order to avert a potential collapse in demand
for Treasuries — an event that he warned would have ‘vicious’ effects. …
U.S. budget experts have for years warned of the potential for a ‘doom
loop,’ where investors start demanding higher yields on Treasuries due
to risks tied to the government’s swelling debt
burden, which then causes an increase in the government’s interest
payments — in turn widening the deficit. … ‘It’s going to take increased
revenues, taxes, and dealing with expenses,’ he said. It would also mean
overhauling Social Security and health care programs, he said. ‘You can
raise the revenues without a big drag on growth, if you close preferences
and loopholes in the tax code.’”
LTC Comment:
Remember when
Modern Monetary Theory told us the U.S. government could spend without
restraint by printing money to fill funding gaps? Whoops! Turns out
there’s a limit to that strategy. When you borrow so much that no one is
willing to loan you more, you’re stuck. This reality is what will finally
force America to confront problems like out-of-control entitlement
spending. The good news is that we have plenty of
realistic solutions to draw from to fix LTC.
LTC BULLET: LTC
INSURANCE FRAUD
LTC Comment:
LTC insurance fraud was a frequent topic at the recent Intercompany
Long-Term Care Insurance (ILTCI) conference in Orlando, Florida. We
covered that conference and its fraud sessions in detail a couple weeks
ago in
LTC Bullet: ILTCI 2026 Virtual Visit.
In the
meantime, your Center for Long-Term Care Reform has started digging deeper
into LTC insurance fraud. We’re especially interested in measures LTCI
carriers have taken to identify, mitigate, and prosecute fraud. We will
conduct a literature search and interview some of the experts who
presented at the ILTCI meeting. We also invite anyone with expertise on
this topic to share your insights and suggestions by contacting
smoses@centerltc.com.
Our special
interest in this topic is to identify best fraud control practices
developed by private LTCI carriers that may be transferable to ameliorate
the much bigger problem in public programs, especially Medicaid and
Medicare. For now, we’re scoping out the general subject of health care
fraud. These are some of the issues, suggested by AI, that we plan to
explore in a draft paper and op-eds.
Insurance
Fraud Incidence
Finding precise, "hard" data for long-term care (LTC) fraud is
challenging because it is often grouped into broader "healthcare fraud" or
"improper payment" categories. However, recent industry reports and
government snapshots provide these estimated figures for 2023–2025:
Private
Sector LTC Insurance Fraud
In the private sector, fraud is often measured as a percentage of
total claims paid.
- Estimated
Fraud Rate: Experts from firms
like illumifin and
the Coalition
Against Insurance Fraud estimate
that 5% to 10% of all LTC insurance claims involve some form of
fraud, waste, or abuse.
- Financial
Impact: With the industry paying approximately $14.1 billion in
benefits in 2023, the estimated annual loss to fraud is roughly $700
million to $1.4 billion.
- Case
Severity: For sentenced healthcare fraud cases in 2024, the median
loss per case was approximately $2.5 million, with nearly 20% of
cases involving losses over $9.5 million.
Health Care Fraud
LTCi becoming more of a target for fraud
What Data Says About Health Care Fraud
Public
Sector (Medicare & Medicaid) LTC Fraud
The public sector primarily tracks "Improper Payment Rates." It
is critical to note that while improper payments include fraud,
they also encompass administrative errors like missing documentation.
Medicare Program Integrity and Efforts to Root Out Improper Payments,
Fraud, Waste and Abuse
Fiscal Year 2024 Improper Payments Fact Sheet
- Medicaid
(FY 2025 Estimates):
-
Improper Payment Rate: 6.12% ($37.39 billion), an increase
from 5.09% in FY 2024.
-
Fraud Specifically:
Of these improper payments, only a fraction is confirmed fraud. Most
(over 77%) are attributed to insufficient documentation.
- Medicare
(FY 2025 Estimates):
-
Fee-for-Service (FFS): 6.55% ($28.83 billion).
-
Medicare Advantage (Part C): 6.09% ($23.67
billion), often due to lack of documentation for diagnoses.
-
Enforcement Outcomes (FY 2024): State Medicaid
Fraud Control Units (MFCUs) reported 1,151 convictions and
recovered $1.4 billion.
5 Key Facts About Medicaid Program Integrity – Fraud, Waste, Abuse and
Improper Payments
Fiscal Year 2025 Improper Payments Fact Sheet
Medicaid Fraud Control Units Annual Report: Fiscal Year 2024
Improper Payments and Fraud: How They Are Related but Different
Types of Corporate Fraud
Fraud
Tolerance
There is evidence suggesting that a
segment of the public, particularly younger generations, has developed a
higher tolerance for certain types of non-violent fraud, such as insurance
fraud and digital scams. While many still view these actions as
illegal, studies indicate a growing trend of rationalizing or accepting
"lower-level" fraud, often viewing it as a victimless crime against large,
wealthy corporations rather than individuals.
Survey Finds Younger Generations Have a Higher Tolerance For Insurance
Fraud – What Insurers Should Know
Fraud Types
Shared by Public and Private Insurers
-
"Phantom"
care and billing: Submitting claims for services never provided, such as
x-rays, drugs, or home
care hours.
-
Upcoding:
Misrepresenting a patient's diagnosis or severity to bill for a higher
rate of reimbursement.
-
Medical
Identity Theft: Fraudsters visiting facilities to collect Medicare or
Medicaid numbers under the guise of offering "free" services, later used
for bogus billing.
-
Kickbacks:
Financial incentives given to physicians or facilities to steer patients
toward specific high-cost therapies
or services.
-
These practices often involve predatory
actors working on both the public and private sides.
Common Red
Flags
- Early
Duration Claims: Claims filed soon after a policy is purchased.
- Unusual
Billing: Inconsistent, high, or rapidly increasing hours.
- Pressure
Tactics: Salespeople rushing decisions or pushing to handle all
documentation.
-
Too-Good-To-Be-True: Policies promising to cover everything.
Around 38.5% of companies surveyed
reported provider misrepresentation of services as a significant risk.
Critical
Vulnerability: Cognitive Impairment
A major finding in current research
is that populations with diminished capacity are disproportionately
targeted. Both private and public sectors are now prioritizing caregiver-specific
audits and specialized training for claim examiners to detect when a
patient is being manipulated into signing falsified
logs or timesheets.
Common LTC Fraud Schemes Targeting Vulnerable Seniors
Private
Sector Lessons Transferable to the Public Sector
Private insurers have pioneered
several strategies that are now considered best
practices for public side
enforcement:
6 Claims Best Practices for Life Insurance Fraud Prevention
The public sector can enhance its
anti-fraud efforts by adopting the private sector’s focus on individual-level
behavioral verification and formalized cross-payer data integration.
While programs like Medicare and Medicaid excel at large-scale algorithmic
detection, private insurers often utilize more "on-the-ground"
investigative techniques that can identify sophisticated schemes where the
billing data itself appears legitimate.
Fraud Control in the Health Care Industry: Assessing the State of the Art
1. Shift
from "Pay and Chase" to Real-Time Prevention
The public sector can adopt private-sector strategies to move from
reactive recovery to proactive prevention:
- Adopting
"Pre-Payment" Edits: Private insurers use sophisticated "claim
scrubbing" applications to flag anomalies before payment is
issued. Implementing similar real-time root-cause analysis in public
systems can reduce the need for expensive post-payment investigations.
-
Electronic Visit Verification (EVV) Optimization: Public programs
can learn from private insurers' use of GPS and biometric data to ensure
caregivers are physically present at the reported care location, a key
defense against "phantom" billing.
Public-Private Partnership to Prevent Health Care Fraud Announced by
Health and Human Services
Best practices for employers to combat claims-related healthcare fraud
Long-Standing State-Based Efforts to Combat Fraud Against Medicaid
Continue to Improve
2. Enhanced
Behavioral and Field Investigations
Private insurers often identify fraud
by looking beyond the billing codes to the actual lifestyle and behavior
of the parties involved:
- Targeted
Surveillance: Private sector "field investigations" frequently
uncover fraud—such as patients performing activities they claim to be
unable to do—that purely data-driven public audits might miss.
-
Caregiver-Specific Audits: Focusing research on the caregiver’s
lifestyle, professional licensing, and historical litigation can uncover
systemic fraud rings.
Long-Standing State-Based Efforts to Combat Fraud Against Medicaid
Continue to Improve
3.
Formalized Information Sharing Networks
Public-private partnerships are the most direct way for the public
sector to benefit from private-sector progress:
-
Healthcare Fraud Prevention Partnership (HFPP): This voluntary
program allows federal and state agencies to share data with private
plans to gain a "cross-payer" view. This helps identify "double billing"
where a provider bills both a private LTC policy and Medicare for the
same service on the same day.
- Unified
Fraud Hotspots: By sharing data on specific suspicious billing codes
and geographic fraud "hotspots," the public sector can direct its
high-intensity enforcement teams more effectively.
About the Partnership
Public-Private Partnership to Fight Fraud Formed
Public-Private Partnership to Fight Fraud Formed
Public-Private Partnership to Prevent Health Care Fraud Announced by
Health and Human Services
4. Improving
Public Awareness and Reporting
The public sector can refine its
"whistleblower" and awareness campaigns by studying what motivates
individuals in the private sector to report fraud:
The Public’s Self-Avoidance and Other-Reliance in the Reporting of Medical
Insurance Fraud: A Cross-Sectional Survey in China
-
Incentivizing Reporting: Research shows a "free-rider" mentality
often prevents people from reporting public insurance fraud.
Strengthening whistleblower protections and creating stronger
incentives—similar to those in private litigation—can improve the flow
of actionable leads to Medicaid
Fraud Control Units (MFCUs).
Long-Standing State-Based Efforts to Combat Fraud Against Medicaid
Continue to Improve
- Education
on Specific Red Flags: Adopting private-sector training that teaches
beneficiaries to look for "red flags" like pre-filled timesheets or
inconsistent care plans can empower them as a front-line defense.
Long-Term Care Fraud (NAIC)
Key Trend:
Both sectors identify Personal Care Services (PCS) as the highest
risk area. In Medicaid, PCS attendants and agencies accounted for the most
fraud convictions (326 in FY 2025), a trend mirrored in private sector
reports identifying home care as a "major industry challenge".
Medicaid Fraud Control Units recover $700,000 in assisted living cases,
with 300+ investigations still open
#############################
Updated
Monday, April 13, 2026, 10:03 AM (Pacific)
Seattle—
#############################
LTC E-ALERT #26-011: LTC NEWS AND COMMENT
LTC Comment: Do you spend hours searching
the internet for useful articles, key data, and relevant reports to keep
you on the forefront of professional knowledge? Do you lose business
because you’re blindsided by clients or competitors who learn critical
information before you do? Here’s an antidote:
LTC Clippings: The Center for Long-Term
Care Reform notifies subscribers to our LTC Clippings service daily of
information you need to know. Each message contains only the critical
facts about new publications: a title, representative quote, a link to
the original, and our analysis in a sentence or two. To inquire or
subscribe, contact Damon at 206-283-7036 or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC E-Alerts: Once a week, we compile our
daily LTC Clippings into a summary, email it to Center for Long-Term Care
Reform members, and archive it in The Zone, our password-protected
members-only website. Center members also receive our weekly LTC Bullet
op-ed. To join the Center and receive all these benefits and more,
contact Damon at 206-283-7036 or
damon@centerltc.com.
We no longer post our LTC E-Alerts on the
Center’s public access website, but here’s what today’s LTC E-Alert
contained: links, quotes and comments on the following articles, reports,
or data:
-
Report: With
spend-down of assets, US long-term care system ‘effectively penalizes
aging’
-
How Long-Term Care
Costs Drain the Middle Class and Deepen Intergenerational Wealth
Inequality
-
Less than half of
Americans are planning for their retirement healthcare needs, survey
finds
-
Skilled nursing
emerging among most attractive real estate sectors
-
Layin’ It on the
Line: The long-term care crisis in Utah: Why national plans fail here
and how to shield your assets (Part 2)
-
Future long term
care expenditure trajectories across OECD countries
-
The Five Biggest
Medicaid Planning Mistakes — and How to Avoid Them
-
Rising Long-Term
Healthcare Costs Pose Growing Threat to Farm Family Legacies
-
Providers must
educate prospects to cut gap between expectations, realities of senior
living rates: report
-
Eight arrested in
$50M hospice fraud scheme as oversight intensifies
#############################
"LTC E-Alerts" are
a
feature offered by the Center for Long-Term Care Reform, Inc. to members
at the $150 per year level or higher. We'll track and report to you news
and analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Monday, April 6, 2026, 10:03 AM (Pacific)
Seattle—
#############################
LTC E-ALERT #26-010: LTC NEWS AND COMMENT
LTC Comment: Do you spend hours searching
the internet for useful articles, key data, and relevant reports to keep
you on the forefront of professional knowledge? Do you lose business
because you’re blindsided by clients or competitors who learn critical
information before you do? Here’s an antidote:
LTC Clippings: The Center for Long-Term
Care Reform notifies subscribers to our LTC Clippings service daily of
information you need to know. Each message contains only the critical
facts about new publications: a title, representative quote, a link to
the original, and our analysis in a sentence or two. To inquire or
subscribe, contact Damon at 206-283-7036 or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC E-Alerts: Once a week, we compile our
daily LTC Clippings into a summary, email it to Center for Long-Term Care
Reform members, and archive it in The Zone, our password-protected
members-only website. Center members also receive our weekly LTC Bullet
op-ed. To join the Center and receive all these benefits and more,
contact Damon at 206-283-7036 or
damon@centerltc.com.
We no longer post our LTC E-Alerts on the
Center’s public access website, but here’s what today’s LTC E-Alert
contained: links, quotes and comments on the following articles, reports,
or data:
-
CMS CRUSH
initiative alone not sufficient to fight fraud, groups say
-
Federal Debt
Management: Treasury Is Meeting Borrowing Needs but the Deteriorating
Fiscal Outlook Poses Risks
-
Home care groups
CRUSH plans for more anti-fraud requirements
-
What Happens When
the Social Security Trust Fund Is Exhausted?
-
Who should pay for
older adults’ care? Caregivers answer differently
-
Waste, Fraud, and
Abuse in Government Health Care Programs is No Joke
-
We Are 63 With
$5.7 Million. My Wife Wants to Buy Long-Term Care Insurance, but I Want
to Self-Insure. Who Is Right?
-
New Medicare HCBS
model, designed for California, targets ‘overlooked middle’
-
Top economist
finds silver lining for skilled nursing amid nation’s uncertain outlook
#############################
"LTC E-Alerts" are
a
feature offered by the Center for Long-Term Care Reform, Inc. to members
at the $150 per year level or higher. We'll track and report to you news
and analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Friday, April 3, 2026, 10:03 AM (Pacific)
Seattle—
#############################
LTC Bullet:
ILTCI 2026 Virtual Visit
LTC Comment: ILTCI ’26 was another successful industry convocation. This
“virtual visit” to the conference is intended to give those who could not
attend a sense of what it was like and to encourage them to consider
attending in the future. It follows the ***news.***
|
*** TODAY'S LTC BULLET is sponsored by Claude
Thau (BackNine Insurance). BackNine gives you a free
personalized website at no cost. Your clients (& family & friends)
can, with as little or as much of your involvement as you or they
want, buy life insurance and LTCi, and can speed issue by scheduling a
paramed and uploading medical records immediately. We quote
stand-alone LTCi, linked-benefit and life with a LTC rider
side-by-side. Claude is the lead author of Milliman’s annual Broker
World LTCi Survey & a past Chair of the Center for Long-Term Care
Financing. Contact him at 913-707-8863 or
claude@back9ins.com to learn about more
great BackNine features and services. *** |
*** HAPPY BIRTHDAY to the Center for Long-Term Care Reform. We completed
our 28th year on April 1, 2026. Check out the Center’s many
state- and national-level policy studies
here. Read dozens of published articles
here. Speeches,
here. Review hundreds of LTC Bullets, organized by topic and
chronologically,
here. This is how we announced our mission in “Center
for Long-Term Care Financing Established; "LTC Bullets" Opening Salvo”:
“The Center will advocate public policy that targets scarce public
resources to the neediest, while encouraging people who are young, healthy
and affluent enough, to take responsibility for themselves. We believe
that private insurance and investment can guarantee quality long-term care
for prosperous seniors and help to save the Medicaid long-term care
program for the truly needy. The Center will offer a range of
fee-for-service products to public and private clients including
consulting, publishing, training and public speaking.” It’s been a great
run and it will continue as long as we have your support and collegiality
in our common mission to improve long-term care for all Americans. ***
LTC BULLET: ILTCI 2026 VIRTUAL VISIT
LTC Comment: The
2026 Intercompany Long-Term Care Insurance Conference convened
March 8–11, 2026 in Orlando, FL at the Rosen
Shingle Creek Resort. The meeting’s theme this year was "Dream… Design…
Deliver: Reimagining the Future of LTC.” Conference chair, Gina Besz from
“illumifin,” opened the proceedings. She told the 1000-plus attendees what
to expect, thanked the organizers, presenters and sponsors, and disclosed
(always a topic of great interest) the city hosting next year’s
conference: Indianapolis, March 14-17, 2027. She also surprised us
by sharing where the meeting will convene the following year: Houston,
April 2-5, 2028.
Next came announcement of the
ILTCI Recognition Award recipients for 2026. This award “honors the
trailblazers, innovators, and lifelong contributors advancing long-term
care insurance and shaping the future of aging in America.” Steve Serfass,
Partner, Faegre Drinker Biddle and Reath, LLP, received the individual
award. Two companies shared the organization award: Lincoln Financial and
One America. Congratulations to these award recipients for their many
years of dedication and hard work in our common mission to improve
long-term care for all Americans.
Jeff Noel, a 30-year Disney Leadership veteran, sponsored by
NGL, keynoted the conference. He's the author of “Mid-Life
Celebration” and hosts the podcast “If Disney Ran Your Life.” Noel
captivated the audience with stories and theories bearing on leadership
excellence, employee engagement, customer service, brand loyalty,
creativity and innovation. Always do “just a little more than what the
customer expects.” Go the “extra inch” not just the last mile. Their
standing ovation demonstrated the audience’s appreciation of his remarks.
The exhibit hall is a highlight of every ILTCI meeting. It is where
attendees convene to eat, drink, visit exhibitors and network. I missed
the opening exhibit hall reception Sunday night due to flight
complications, but I attended the breakfast, lunch, and late-afternoon
sessions on the remaining two days. To meet, greet, confer, pitch,
negotiate and generally do business of any kind in the LTC insurance
industry, there is nothing like the ILTCI conference with its exhibit hall
and the ample opportunities to connect in the hallways as well. Be there
next year in Indy if you can.
After Monday morning’s announcements and keynote address, the conference
turned to breakout sessions. These included presentations on seven
different subject tracks:
-
Sales, Marketing, &
Distribution: Focused on consumer engagement, expanding into
middle-income markets, and distribution trends.
-
Actuarial & Finance: Covered
topics such as AI in actuarial work, asset-liability management, and in
force management.
-
Management & Operations: Addressed
operational excellence, technology adoption, and call center evolution.
-
Wellness & Aging in Place
Solutions: Explored innovative services, technologies for aging in
place, and AI/robotics in care.
-
Claims & Underwriting: Focused
on accelerated underwriting, electronic health records, and fraud
detection.
-
Legal, Compliance & Regulatory: Covered
regulatory changes, compliance issues, and legal developments impacting
LTC insurance.
-
[Track Name Varies -
General/Future Trends]: Covered broader industry topics, such as the
future of LTC and caregiver crises.
It seems like themes run through the ILTCI conferences for years at a
time. I noted the focus on wellness in
LTC Bullet: Virtual Visit to ILTCI 2023. Emphasizing wellness and
doing more for policyholders than simply processing and paying claims
remains a strong conference theme. But it seemed to me that at the 2026
program fraud identification, control, and mitigation took a new and
bigger role. That topic especially interests me as fraud is soaring right
now in public programs like Medicaid and Medicare. So you’ll see in what
follows that I covered several breakout sessions aimed at the topic of
fraud.
It’s worth noting that another theme, prominent in earlier ILTCI meetings,
has disappeared. That is the public policy context in which the LTC
insurance industry operates. Medicaid is the predominant payer for LTC in
the USA. It crowds out private LTC insurance by desensitizing the public
to LTC risk and cost leaving private LTC insurance with a small residual
of the market. Yet Medicaid was barely mentioned at the 2026 conference.
Even state experiments with public LTC financing such as WA Cares in
Washington State and the latest proposal for a national LTC financing
program, WISH, were mostly ignored. Of course, I wasn’t in every session,
so maybe there was public policy content I missed, but with no track
dedicated to the subject as in the past, its importance has clearly
declined.
First Breakout Monday, March 9, 2026, 10:45am
Track: Legal, Compliance & Regulatory
Title: The Fraud Escape Room Experience: LTC Edition
Description: Step into the world of long-term care insurance fraud
investigations—like you’ve never experienced before. This interactive
session combines real-life case studies with an escape-room-inspired
twist. Our expert panel will guide you through actual fraud investigations
from across the country, highlighting the tactics and techniques used to
uncover and stop bad actors. But beware: after each case, you’ll receive a
cryptic clue left behind by a fictional mastermind who may be
orchestrating these schemes. Are these cases truly unrelated, or is
someone pulling the strings from the shadows? Work together to solve
riddles, connect the dots, and uncover the truth before time runs out.
Join us for a session that educates, entertains, and challenges your
investigative instincts—because in this room, every detail matters.
Moderator:
Matt DeLong, illumifin
Presenters:
Tara Dickson, Cozen O'Conner
Adam Haque, John Hancock
Tom Kakos, illumifin
Matt Keeling, Unum
Comments: This program blew me away. I had no idea fraud was so
rampant in private LTC insurance, nor did I know anything about the highly
creative efforts carriers are employing to identify, prove, and control
fraud that these speakers shared. They described three case studies, each
of which was nearly beyond belief. They told of policy holders who claimed
severe need, got approved, but were then shown to be fully capable of
doing all the ADLs they claimed to be unable to manage. Arrogant and
brazen, the fraudsters evaded being caught until they were shown to be out
of compliance by clever methods described by these presenters. Such
techniques included desktop investigation, searching social media,
unmanned surveillance, tracking travel and many more.
Here’s just one of the anecdotes they shared. Married couple on claim
since 2023. Both filed and approved for similar conditions. Tax qualified
policies. Both had $380 per day home health unlimited lifetime. Both
claimed they needed assistance with five out of six ADLs. Neither claimant
had precipitating event. 12 hours a day 7 days a week for husband. 16
hours for wife. On claim same year. Documentation issues. Desktop
investigation. Social media. Husband was sole owner of home care agency.
Both reported not driving, using cane. Too consistent. Handwriting gave
them away. The same individual did all the documentation. Extremely clever
in how projected. Reviewers struck gold in social media, found something
interesting. Extensive overseas trips while on claim, including Spain,
Portugal, Puerto Rico, California. How could they do that while on claim?
Are caregivers actually showing up? Got video taking trash out with no
trouble, walking with no cane. Wife shopping loading, stuff in vehicle.
All while claiming many hours of care. All activities while caregiver
supposedly providing care. Did 15 days of surveillance. Never saw a single
caregiver come. Interview. Time to talk to claimant. What did you do
today, yesterday? Called and talked to husband. Insisted both need claims,
can’t leave home without caregiver. Are caregivers present? Yes, but just
stepped out to get lifesaving medications.
Showed him all documents, pressed further, eventually admitted he created
all the documentation including the claims. Said took caregivers along on
international trips. Should be records of this. Showed clips of him and
wife moving independently. We’re always in pain, they said. Where are your
caregivers? Biggest turn of investigation. Caregivers returned from
errands. Did not see anyone from our surveillance. No photo IDs. Husband
answered all their questions. Week later, called husband back. He admitted
in Philippines. Who were those individuals claimed to be caregivers? Just
locals from Philippines. Case outcomes. Both claims reviewed by medical
staff. Claims closed. Fraud, waste and abuse reported to Dept. of
Insurance. Settlement reached. Surrendered both policies and made some
repayment.
Second Breakout, Monday, March 9, 2026, 2pm
Track: Legal, Compliance, & Regulatory
Title: Inside the Jury Box: An LTCI Mock Voir Dire, How Everyday
Consumers View LTC Insurance
Description: What do everyday consumers really think about
long-term care insurance—and how might those views shape the outcome of a
trial? In this interactive session, we’ll stage a mock voir dire (jury
selection) to explore how potential jurors respond to key concepts like
policy language, benefit triggers, and product design. Participants will
observe and engage with the process as attorneys question mock jurors,
uncover biases, and strategize selections. Beyond the courtroom drama,
this session offers a rare opportunity to hear unfiltered consumer
attitudes toward LTC insurers, coverage expectations, and claims disputes.
Whether you're in legal, compliance, product, or risk, you'll walk away
with a deeper understanding of how your decisions may be interpreted by a
jury—and how to prepare for it.
Moderator:
Gina Fortin, Unum
Presenters:
Matt Kops, Blueprint Trial Consulting
Chris Petillo, Faegre Drinker
Michael Rafalko, Cozen O'Connor
Comments: Clever idea. Attorneys for the plaintiff and the
defendant interviewed “jurors” playing various roles to represent
different kinds of consumers. Jurors bring experiences, attitudes/values
and personalities to court. A “jury consultant” commented on the process
of selecting or rejecting jurors in the voir dire process of a trial. All
9 jurors interviewed by both attorneys based on a hypothetical complaint
fact pattern. Each attorney eliminated three jurors based on brief
4-minute interviews leaving three of the nine empaneled. The session used
audience polling. The idea was to tease out consumer attitudes about LTC
insurance, but the jurors were all people in the business. So I’m not sure
that objective was achieved. But the session definitely invited
consideration of complex ideas and attitudes about the product.
Third Breakout, Monday, March 9, 2026, 3:45pm
Track: Wellness & Aging in Place Solutions
Title: Imagineering Aging with a Gen Z Advocate: Promising Models
and Interrogational Collaboration
Description: In this fireside chat led by Gen Z advocate Arielle
Galinsky, we'll explore bold ideas for aging-in-place, LTC policy reform,
and the importance of multigenerational collaboration. Arielle brings her
deep passion on all things aging & LTC as well as her commitment to
advancing aging policy reform at the state and national levels. From her
research and experience, she will lead insightful conversation on 1) why
aging needs to be an intergenerational conversation, 2) what we can learn
from international aging models and policies, 3) and what policymakers
need to know to make this vision a reality. Get ready for an energizing
conversation that brings a fresh, forward-thinking perspective on aging.
Speakers:
Cailyn Canty, Davies
Arielle Galinsky, The Legacy Project, Inc.
Comments:
This session was intended to bring to light the innovative perspectives of
a Gen Z influencer. The principle speaker, Ms. Galinsky, was articulate
and knowledgeable. Her views were grounded in personal experience. She
became a Certified Nursing Assistant (CNA) to understand better the
challenges of caregiving. Very thoughtful, but I discerned little unique
perspective from the younger generation. She seemed to be saying what
older generations are also saying with little new analysis. A promising
wrap up to the conversation was promised. But it amounted to referencing
states that have proposed new policy models like WA Cares. What is one
thing we can all do? Support the WISH Act; advocate for it. This is not
fresh thinking, only restating the current public policy thinking, such as
it is in the LTC insurance business.
2nd day March 10, 2026, 9am
Track: Claims and Underwriting
Title: The Current Anti-Fraud Landscape: Industry Insights
Description: Join leading experts as they share how carriers are
currently viewing and addressing fraud. This session will dive into the
latest industry survey findings, examine innovative approaches to fraud
mitigation, and explore effective models for managing fraud, waste, and
abuse (FWA). Attendees will gain valuable perspectives on current
challenges and best practices to safeguard the integrity of LTC claims.
Moderator:
Roy Christenson, ERAC
Speakers:
Jeff Ferrand, illumifin
Jessica Loesing Gallagher, Faegre Drinker
Tom McManama, PwC
Comments: Fascinating session. Fraud recognized as a problem 20
years ago, but over the past 10 years it has really taken off. No longer
lost in a claims “black box.” Fraud identification and control is getting
more sophisticated. Rapid acceleration of technology. Trying to leverage
it. Fraud thought to affect other business lines, but now seen to hit LTC
insurance too. PwC Anti-Fraud Survey showed 6 to 8% of claims have fraud.
$1.3 billion. By 2030 Milliman found $25 billion claims in four years. So
$2.5 to $3 billion in fraud. “We are all fraud ambassadors now.” Much
higher for home health care than these estimates that are across all
products. What is most common type? Claimant and provider fraud and
combination, collusion. Not eligible at start or became not eligible but
stayed on claim. Provider bills where not providing care. Skimming. Charge
for more and pocket some. Easier to investigate home health care (HHC) so
tend to start there. Facility fraud has lot of checks and balances.
Vulnerability in billing practices. Little prosecution of fraud.
Prosecutors focus on bigger fish, like Medicare and Medicaid. The Centers
for Medicare and Medicaid Services (CMS) are only now beginning to search
for and control fraud that runs rampant in public programs but receives
little attention from states that reap a bonanza of federal funding.
2nd day March 10, 2026, 10:45pm
Track: Management & Operations
Title: AI Fakes and Real Risks: Securing Long-Term Care Systems
from Manipulation
Description: As deep fake technology becomes more sophisticated,
the long-term care industry faces new threats to operational integrity and
patient safety. This session explores how AI-generated falsifications can
impact critical areas such as HR, policy administration, and claims
—posing risks to claims processing and regulatory compliance. We’ll
examine real-world scenarios, discuss detection strategies, and explore
how organizations can safeguard against manipulation while maintaining
trust and accuracy in their data systems.
Producer (non-participant):
Paul Marquez, Diligence International Group, LLC
Speakers:
Karen Babio, Davies
Kevin Glasgow, Diligence International Group
Comments:
Overview: Fakes not new, old theme, me toos, art of deception. AI to
create fakes, creating synthetic identities, tech and tools; is your
insurer ready? Most people are honest but some aren’t. Out there to
defraud in any way they can. Have to be careful because there are bad
actors. What is a deep fake? Universal studios pioneered computer
generated voice or image to look real. Systems learn from each other
improving deep fakes. Trojan horse. New tools lowered cost and skill
needed. Art of deception: cognitive biases, shortcuts, emotional
influence, social trust, cooperation, cognitive overload tendencies for
over confidence, expertise gaps. They only have to be right a small
percent of time. Criminals targeting. Awareness gap. Tech gap. What’s
changed? Presenters created the introductory fake very easy, low level. No
tech training. Very low cost to create avatar. Could have done anyone in
the room.
“Catch me if you can”: movie. Impersonations.
Major insight: Change in attitude toward nonviolent crime. Younger
generation much more accepting of profiting from nonviolent crime.
Consider in context of home health fraud. Effect on jury pools.
Fakes are nothing new. Just new tech doing more things. Voting on which
images real. About random chance. Better at finding video fakes.
Using AI fakes to make better, smarter, faster. Phishing, spear phishing
(targeted), vishing (video phishing), smishing (using fraudulent texts).
Counterfeit compliance certs insurance certificates.
Financial records, invoices paystubs, utility bills tax form, fake ID
documents.
Possible imposter originated scams initiators and facilitators: family
members, people in position of trust, insurance community members, human
traffickers, organized crime groups, paramedical examiners, attorneys,
brokers, investors. Getting more organized.
Has your organization any training for deep fakes? What kind?
Apply for credit over and over again. Loyalty information. Gradually
create identify. Get higher and higher credit rating. Fictitious person.
Continue to “ripen” ID until accepted.
AI fraud surges 195%. AI arms race. Synthetic identities. $30 billion in
life insurance industry annually.
Companies need to think more like banks.
Threat actors always out there. Attitude shapes moral compass against
insurers. Insurance has a high ROI. Organized crime funding has entered
the fray.
SIFT: Stop, investigate, find, trace to original source.
2nd day March 10, 2026, 2pm
Track: Management & Operations
Title: Inside the Mind of a Hacker: Cyber security Threats and
Defenses in Insurance
Description: Join an ethical hacker for a behind-the-scenes look at
how cybercriminals are evolving - and how AI is reshaping the cyber
security landscape. Through real-world examples and expert insights, this
session reveals common vulnerabilities, emerging AI-driven attack methods,
and practical defenses. Learn how cyber security impacts your business -
and walk away with actionable strategies to protect your organization from
the risks of an AI-enabled threat environment.
Moderator: Christie Conway, Wellcove
Speakers:
Kalin Kelly, Continental General
Tom Liston, Bad Wolf Security
Comments: AI is not experimental, it’s in the wild. Changing rules
for defenders and offenders. What is AI? Systems that find patterns,
massive data sets, on internet. Lots of knowledge. But dark side. Models
mimic understanding brilliantly. But they don’t reason. Excel at static
prediction not logical deduction. Content generation, code assistance,
customer service, and everything else. Private investment in generative AI
soaring. $34 billion, up 19%. Limits of today’s AI, not necessarily going
to get same output every time. May confidently present but it is wrong.
Not responsible for anything. Falls on humans to control. 4.4% 2023
performance 71.7% 2024 performance. AI coding capability has gone
explosive in growth. Hackers faster, defenders smarter. Fraud pattern
detection. Synthetic employees, when agents talk to agents. Undercurrent.
Sub layer underneath humans. Unmonitored. Could proliferate bad
information. Driven social engineering. Excellent impersonalization. Video
calls. Texts. Email. Phone. Fake documents. Executive impersonalization.
Uncomfortable truth. What companies doing. Not a lot. 78% use, 40%
mitigate risk, 37% have governance. Adoption has exploded, but governance
last.
97% no access controls, 63% no governance. Average global breach cost:
$4.4 million.
Tom Liston: I’m a thief. Broke into banks and much else. 60% of firms
suffered data breach; 277 days to discover a data breach; Overall 93%
resulted in an external attacker gaining internal network access. He set
out to find one compromised business per day. Found 500. Very easy. Who?
Small to medium business, large well-known companies, government
organizations; universities. Solutions: Treat network as if it is
compromised; Limit damage attacker can do, network security basics not
magic black box. Use multi-factor identification. Monitor closely.
2nd day March 10, 2026, 3:45pm
Track: Claims & Underwriting
Title: Game On: Integrating FWA Programs into the Claims Process -
A Chutes and Ladders Experience
Description: Join us for an engaging and interactive session that
brings the classic board game Chutes and Ladders to life. This dynamic
experience combines audience participation with practical insights,
guiding you through the highs and lows of integrating FWA programs into
the LTC claim process. Each “move” on the board represents real-world
examples, challenges, and opportunities - including emerging technologies,
digital controls, smart workflows, and human insights. Led by seasoned
claims executives and an experienced trial attorney, this session goes
beyond theory—offering actionable strategies, risk mitigation tips, and
legal perspectives that matter. Whether you climb the ladder of success or
slide down a chute of unexpected complications, you’ll leave with a deeper
understanding of how to stay ahead in today’s evolving long-term care
claims landscape.
Moderator:
Jane Bagley, Fuzion
Speakers:
Andrew Azarmi, Dentons
Laurene Polignone, John Hancock Financial Services
Kristen Sewell, Continental General
Comments:
Series of scenarios offered. Then vote on whether fraud or not. Go down a
chute if wrong; up a ladder if correct. In the middle, I noted “So far all
examples obvious.” Andrew, the attorney, comes at it from a different
perspective. Lawyer, not insurance company. Lessons learned. Facts in
claims can become questionable. Policyholder appeals claim denial. Submits
signed letter from primary care physician Dr. Feelgood. Under his care.
Suffers cognitive impairment. Needs assistance with several ADLs .You
verify Dr. Feelgood is a board certified MD. Video surveillance over 5
days reveals policyholder is walking, driving, entering/exiting sedan,
rolling 2 large trash cans from curb up sloped driveway into garage.
Picking up dry cleaning while talking on cell. Entering and exiting
Pilates studio. Answer: Time review.
3rd Day, March 11, 2026, 8:30am
Title: Alzheimer's Association: Explore Cutting-edge Developments in
Brain Health, Diagnosis, and Treatments
Description: Learn how lifestyle interventions can reduce the risk
of cognitive impairment, how blood-based biomarkers are enabling earlier,
more accessible Alzheimer’s diagnosis and advancements in treatments. The
second half of this session will provide a comprehensive overview of
rapidly moving innovations within dementia care specialty models including
both Medicare and Medicare Advantage funded approaches. The impressive
early clinical and cost savings outcomes and how LTCI specifically might
take advantage in the short-to-mid-term. Discussions will include an
overview of the Dementia Care Navigation Service, powered by Rippl and the
Alzheimer’s Association, which has shown promising results including a 30%
drop in emergency department visits and a 15% reduction in hospital
admissions through personalized, proactive support aligned with Center for
Medicare and Medicaid’s GUIDE Model.
#############################
Updated
Monday, March 30, 2026, 10:03 AM (Pacific)
Seattle—
#############################
LTC E-ALERT #26-009: LTC NEWS AND COMMENT
LTC Comment: Do you spend hours searching
the internet for useful articles, key data, and relevant reports to keep
you on the forefront of professional knowledge? Do you lose business
because you’re blindsided by clients or competitors who learn critical
information before you do? Here’s an antidote:
LTC Clippings: The Center for Long-Term
Care Reform notifies subscribers to our LTC Clippings service daily of
information you need to know. Each message contains only the critical
facts about new publications: a title, representative quote, a link to
the original, and our analysis in a sentence or two. To inquire or
subscribe, contact Damon at 206-283-7036 or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC E-Alerts: Once a week, we compile our
daily LTC Clippings into a summary, email it to Center for Long-Term Care
Reform members, and archive it in The Zone, our password-protected
members-only website. Center members also receive our weekly LTC Bullet
op-ed. To join the Center and receive all these benefits and more,
contact Damon at 206-283-7036 or
damon@centerltc.com.
We no longer post our LTC E-Alerts on the
Center’s public access website, but here’s what today’s LTC E-Alert
contained: links, quotes and comments on the following articles, reports,
or data:
-
My brother says lawyers can get him a Medicaid
nursing home in Florida for a ‘hefty fee,’ despite his assets. Is this a
scam?
-
Family caregivers’ unpaid work valued at over $1T
in 2024, AARP report finds
-
China launches long-term care insurance system to
alleviate aging challenges
-
Long-term care is expensive. Take these 3 steps now
to help you afford it later.
-
Fears Over Retirement Healthcare Costs Are Rising —
And Many Americans Aren’t Planning for Them
-
A Medicaid 'spend down' may get an older person
long-term care coverage but isn't a DIY strategy
-
5 ‘AI-proof’ healthcare jobs will surge through
2034
-
Lincoln Financial Recognized for Leadership in the
Advancement of Long-Term Care Planning
-
Japan's elder-to-elder caregiving crisis fuels
homicides and hidden neglect
-
‘Heartbreaking and destructive’: Ohio lawmakers
seek to rein in Medicaid home liens
#############################
"LTC E-Alerts" are
a
feature offered by the Center for Long-Term Care Reform, Inc. to members
at the $150 per year level or higher. We'll track and report to you news
and analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Wednesday, March 25, 2026,
10:03 AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #26-008: LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Senior care rates balloon in every state: CareScout
report
-
Older adults with financial trouble experience
faster cognitive decline, study finds
-
CMS’ anti-fraud tactics run risk of destabilizing
HCBS system, article asserts
-
Alzheimer’s beneficiaries benefited from Medicare
Advantage risk adjustment model, study finds
-
Lawmakers reintroduce Hospice CARE Act, which would
update benefit, help stop fraud
-
UPDATED: ‘Good news’ as CMS doubles spending on
nursing home staffing campaign
-
2026 Long-Term Care Market Outlook
-
Simultaneous senior care and child care burdening
‘sandwich generation,’ report finds
-
State scraps managed care for Medicaid’s LTC
patients
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Monday, March 23, 2026, 10:03 AM (Pacific)
Seattle—
#############################
LTC BULLET: VINCE BODNAR ON LUMOS
(corrected)
LTC Comment: Today’s “Guest Bullet” features Vince
Bodnar with exciting Plateau/Lumos developments after the ***news.*** (We
regret having accidentally published an earlier, unedited version of this
material on Friday, March 20.)
*** THE 2026 ILTCI CONFERENCE in Orlando, Florida
March 8-11 was another big success. Over 1000 attendees explored LTCI’s
frontiers in each of
seven subject tracks. The Center for Long-Term Care Reform will bring
you our annual “virtual visit” to the 2026 conference in two weeks. Our
conference coverage, giving summaries of the program’s keynote and
breakout sessions, is a tradition that goes back to the first one in
Miami, 2001. Check out our “History
of the LTC Insurance Conferences” published in 2021 and for conference
coverage 2023 to 2025, search “virtual”
here. These sources offer a fascinating history of the hot topics and
many challenges the industry has faced year-by-year during the first
quarter of the current century. Enjoy! ***
LTC BULLET: VINCE BODNAR ON LUMOS
(corrected)
LTC Comment: I’ve followed the long-term care
insurance industry’s successes and challenges since the mid-1980s. Through
most of that history one name stood out for his expertise, creativity,
professionalism and congeniality. Vince Bodnar has concentrated on LTCI
since 1990. With over three decades of experience, he has held many key
roles, including Chief Actuary at illumifin, co-founder of DaVinci
Consulting Group, LLC, and leadership positions at Genworth Financial,
Willis Towers Watson and Milliman. He has spent his career shaping how
America understands and delivers long-term care protection. He has thrice
chaired the ILTCI Conference, founding its Wellness & Aging in Place
Solutions Track during his last chairmanship, twice chaired the Society of
Actuaries LTC Section and founded what is now the LTCi Consortium. He has
also been recognized for his contributions to LTC insurance program design
on multiple continents.
From his early actuarial work designing innovative
coverage models to his leadership in advancing new distribution strategies
across the LTC industry, Bodnar has been a consistent voice for
disciplined, sustainable product development. Now, as President of The
Plateau Group – recently rebranded as Lumos Insurance—he’s applying that
same clarity of purpose to a broader challenge: integrating long-term care
into the full retirement journey.
Bodnar's arrival at Lumos comes at a pivotal moment.
The 45-year-old carrier is building a suite of senior-focused life,
health, and long-term care solutions—each grounded in the company's
hallmark underwriting rigor and long-term risk discipline. For Bodnar, the
mission is not just to launch products, but to redefine how retirees and
their advisors approach aging, income, and care as connected parts of a
single financial story.
Here in his own words is what Vince Bodnar and Lumos
seek to achieve.
Building LTC into a Lifecycle: How a 45-Year
Credit Insurance Carrier Is Entering the Senior Market
You don’t expect conversations about long-term care
planning to begin with credit insurance, but that foundation is central to
understanding what Lumos is now building in the senior market. The Plateau
Group was founded in 1981 by a consortium of Tennessee banks as a credit
insurance carrier. Under that name, it spent more than four decades
helping lenders manage portfolio risk responsibly.
In March 2026, the company rebranded as Lumos
Insurance. The new name follows a multi-year modernization of the
company’s operating infrastructure and governance framework. The overhaul
was significant enough that its leaders decided a new brand was necessary
to reflect the changes.
That modernized platform is broader than the old name
suggested. Lumos now spans senior-focused life and health solutions,
supplemental health products, and specialty property and casualty
programs—in addition to the credit insurance work that started it all. The
company holds an AM Best A- (Excellent) financial strength rating and has
maintained it through more than four decades of market cycles.
The part of that platform getting the most attention
right now is the senior market. Specifically, what Lumos is building
around long-term care.
"Insurance is a long-duration business. Clarity
early — around objectives, product design, distribution structure, and
accountability — allows execution to scale responsibly." — Vince
Bodnar, President & CFO, Lumos Insurance
Meeting People Where They Are in Retirement
Getting older is expensive. Medicare covers a lot,
but not long-term care—and that gap can swallow a retirement plan fast.
Lumos is building a suite of products, all backed by large global
reinsurers, aimed at helping people manage that exposure, starting in the
second half of 2026.
The company’s philosophy starts with a simple
observation: the industry has long treated Medicare supplement coverage,
retirement income, and long-term care as three separate conversations,
usually with three different advisors. Lumos is trying to change that. The
goal is to give agents a way to start a relationship with a client at
retirement and stay useful to them as their needs change over the
years—being there for the wellness questions, the family stress, and
eventually the care itself.
The entry point is a Medicare supplement product for
clients who are newly eligible for Medicare. From there, Lumos plans to
introduce a long-term care product suite that covers multiple types of
buyers and distribution models—traditional standalone LTC coverage,
products designed for worksite or direct-to-consumer channels, and hybrid
structures that pair longevity protection with care funding.
One product is already on the market and is gaining
traction. Lumos has introduced an underwritten single-premium immediate
annuity—a SPIA—designed specifically for people who are already receiving
care and need more income to cover it. The problem it solves is real:
someone in a care facility, burning through savings, who needs a
predictable income stream to avoid outliving their money. The product is
available in several states now and is expected to reach most states
within 30 days.
Lumos is also looking beyond traditional insurance
products. The company is evaluating ways to help retirees tap home equity
to support aging in place—modest home modifications, safety technology,
the kind of investments that let someone stay in their own house longer.
It’s not insurance, but it addresses the same underlying goal.
The proposed suite also includes wellness support,
caregiver resources, and care coordination services. That last piece
matters more than it might sound. Most long-term care is delivered by
family members—a daughter driving her mother to appointments, a spouse
managing medications, a son trying to figure out what Medicaid does and
doesn’t cover. Lumos wants to give those families practical tools, not
just policyholders a policy.
For agents and advisors, the model is designed around
continuity. An agent who writes a Medicare supplement policy at 65 has a
natural reason to come back at 70, and 75, and beyond—if the carrier has
products worth coming back for. That’s the relationship Lumos is trying to
make possible.
Credit Insurance Is Still the Core
"Credit life, health, property and related remain
core to our identity, but our platform is broader. The underwriting rigor
that built our credit business now applies equally to senior health,
supplemental health, and specialty P&C programs." — Vince Bodnar
None of this means Lumos is walking away from credit
insurance. The company is emphatic on that point. Credit protection isn’t
a legacy business being maintained out of nostalgia—it’s the foundation
everything else is built on. And the credit-driven insurance market, it
turns out, needs disciplined carriers right now. Many larger companies
have pulled back from credit life, credit health, and related products in
recent years. Lumos has moved toward that gap rather than away from it.
The three pillars of the Lumos platform—Credit
Protection, Specialty Property & Casualty, and Life & Health—run on the
same operating discipline. The governance standards, the underwriting
rigor, the commitment to long-term partner alignment: those aren’t new.
They’re just being applied to new markets.
What Comes Next
The full product suite is expected to roll out
through 2026, with specific timing dependent on regulatory approvals state
by state. Lumos says more details will emerge as the year progresses. The
bigger idea behind all of it is straightforward, even if the execution is
complicated. People need help at the beginning of retirement, in the
middle of it, and at the end of it—and those needs are connected. A
carrier that can stay relevant across all three stages is more valuable
than one that shows up once and disappears. For a company that spent 45
years staying close to borrowers through the life of a loan, that
philosophy should feel familiar. The product just looks different now.
#############################
Updated Tuesday, March 17, 2026,
10:03 AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #26-007: LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Medicare Advantage Reallocates Subsidies
from the Sick to the Healthy
-
The Looming Crisis in Home Health Care
-
AARP Report Finds Long-Term Care Costs
Outpacing Americans’ Incomes
-
OneAmerica Financial earns national LTC
award
-
Reimagining long-term care through AI
-
Local Governments Play An Important Role In
Medicaid Financing
-
[Column] Direction and Challenges of
Long-Term Care Insurance System Reform
-
WA Cares needs to clarify family caregivers
needn't be union members
-
Medicare Advantage: 14 Steps to a Better
Program
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Monday, March 9, 2026, 10:03 AM (Pacific)
Seattle—
#############################
LTC E-ALERT #26-006: LTC NEWS AND COMMENT
LTC Comment: Do you spend hours searching
the internet for useful articles, key data, and relevant reports to keep
you on the forefront of professional knowledge? Do you lose business
because you’re blindsided by clients or competitors who learn critical
information before you do? Here’s an antidote:
LTC Clippings: The Center for Long-Term
Care Reform notifies subscribers to our LTC Clippings service daily of
information you need to know. Each message contains only the critical
facts about new publications: a title, representative quote, a link to
the original, and our analysis in a sentence or two. To inquire or
subscribe, contact Damon at 206-283-7036 or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC E-Alerts: Once a week, we compile our
daily LTC Clippings into a summary, email it to Center for Long-Term Care
Reform members, and archive it in The Zone, our password-protected
members-only website. Center members also receive our weekly LTC Bullet
op-ed. To join the Center and receive all these benefits and more,
contact Damon at 206-283-7036 or
damon@centerltc.com.
We no longer post our LTC E-Alerts on the
Center’s public access website, but here’s what today’s LTC E-Alert
contained: links, quotes and comments on the following articles, reports,
or data:
-
Number of hospice
enrollees increased last year for third year in a row, report finds
-
In 2025, number of
home health agencies ticked up, bucking trend, new chartbook says
-
America’s Dementia
Care Crisis
-
CMS targets New
York for home care fraud
-
Assisted living
sees highest year-over-year growth compared with other areas of
long-term care
-
5 Retirement
Planning Tips for Solo Agers
-
‘Excellent
evidence’ nursing home staffing mandates don’t cause financial harm:
study
-
Unlocking Idle
Annuities
-
1 in 5 older
adults would pick assisted living if they no longer can live alone: Pew
survey
#############################
"LTC E-Alerts" are
a
feature offered by the Center for Long-Term Care Reform, Inc. to members
at the $150 per year level or higher. We'll track and report to you news
and analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Monday, March 2, 2026, 10:03
AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #26-005: LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Genworth's CareScout Unit Jumps Into the Aging
Crisis
-
Recent Medicaid data release has research
limitations, home care advocates say
-
Understanding Medicaid Home Care Amid CMS Focus on
Potential Fraud and Abuse
-
Long-term care insurance mergers & acquisitions –
What have we learned since 2023?
-
Economic uncertainty challenges retirement
confidence among older adults: survey
-
As aid-in-dying laws come to more states, nursing
homes face tough new decisions
-
NGL launches new long term care product
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Friday, February 27, 2026, 10:03 AM (Pacific)
Seattle—
#############################
LTC BULLET: SO WHAT IF THE GOVERNMENT PAYS FOR MOST
LTC, 2024 DATA UPDATE
LTC Comment: Heads up! We're about to explain why
long-term care insurance sales have disappointed, why people don't "use
their homes to stay at home" and why LTC providers who depend on public
financing are at risk. Details after the ***news.***
|
*** TODAY'S LTC BULLET is sponsored by Claude
Thau (BackNine Insurance). BackNine gives you a free
personalized website at no cost. Your clients (& family & friends)
can, with as little or as much of your involvement as you or they
want, buy life insurance and LTCi, and can speed issue by scheduling a
paramed and uploading medical records immediately. We quote
stand-alone LTCi, linked-benefit and life with a LTC rider
side-by-side. Claude is the lead author of Milliman’s annual Broker
World LTCi Survey & a past Chair of the Center for Long-Term Care
Financing. Contact him at 913-707-8863 or
claude@back9ins.com to learn about more
great BackNine features and services. *** |
*** ILTCI CONFERENCE: The big annual LTC insurance
conference is coming up March 8-11 at the Rosen Shingle Creek Resort in
Orlando, Florida. Get all the latest information
here. You’ll find the
Session Schedule Matrix, and information on the
Keynote Speaker, the
Alzheimer’s Association Session, and much more. Read the
session descriptions and get a general conference
schedule outline. Get details on the
CLTC Master Class and the
Future Leaders Program. Organizers say:
Over the past 25 years: The ILTCI Conference has
grown to be the nation’s largest gathering of the extended care
industry’s top thought leaders. Professionals from all disciplines
attend and participate in a concerted effort to broaden their knowledge,
network, and bring more consumers to the table to plan for their long
term care needs. Contributors and speakers share cutting-edge expert
opinions and analysis covering diverse fields in our 7 tracks while
exhibitors and sponsors showcase a broad range of solutions and
advancements.
Register
here.***
LTC BULLET: SO WHAT IF THE GOVERNMENT PAYS FOR MOST
LTC, 2024 DATA UPDATE
LTC Comment: Once a year, the Centers for Medicare
and Medicaid Services (CMS) reports health care expenditure data for the
latest year of record. In January, CMS posted 2024 statistics on its
website
here. Click on this link
NHE Tables (ZIP) to download the tables. Then, click on the ones of
interest, Tables 13, 14 and 15 for our purposes here.
Health Affairs has published a summary and
analysis of this new data titled “National
Health Care Spending Increased 7.2 Percent In 2024 As Utilization Remained
Elevated." The article is “open access” so available free
here. Unfortunately, the Health Affairs article has little to
say about long-term care beyond the raw data. This was the extent of it:
In 2024, mainly as a result of declining
enrollment, all Medicaid services except home health care and nursing
and residential care facilities experienced growth that was slower than
growth in 2023. … Services used for long-term care (the population most
likely to use this type of care was more likely to retain Medicaid
coverage)—including other health, residential, and personal care
services; home health care; and nursing and continuing care retirement
communities—continued to experience strong growth in 2023 and 2024
(8.9 percent and 9.5 percent, respectively; data not shown).
Not much on LTC, but more than in past years. Note
the surge in nursing home, home care, and residential care expenditures.
Read on to get the rest of the story.
Following is our annual analysis of the latest
long-term care expenditure data. Note that we added Table 13, “Other
Health, Residential, and Personal Care Expenditures,” to our analysis
starting two years ago. This category includes Medicaid home and community
based waivers and care provided in residential care facilities, so it is a
vital part of the LTC marketplace. We focused only on nursing home[1]
and home health expenditures before.
Heads Up: This may be the most important
LTC Bullet we publish all year. It is the twenty-fourth in a row we’ve
done annually to analyze the federal government’s enormous, and we argue,
often detrimental, impact on long-term care financing. If you'd like to
see the earlier versions, go
here and search for “So What if the Government Pays.” You’ll find our
yearly analyses of the data going all the way back to "So
What If the Government Pays for Most LTC, 2002 Data Update."
------------------
"So What If the Government Pays for Most LTC, 2024
Data Update"
by
Stephen A. Moses
Ever wonder why LTC insurance sales and market
penetration are so discouraging? Or why reverse mortgages are rarely used
to pay for long-term care? Or why LTC service providers are always
struggling to survive financially and still provide quality care? Read on.
Nursing Homes
America spent 219.9 billion on nursing facilities and
continuing care retirement communities in 2024, a 7.3% increase compared
to 2023. The percentage of these costs paid by Medicaid and Medicare has
gone up over the past half century (from 26.8% in 1970 to 57.4% in 2024,
up 30.6% of the total) while out-of-pocket costs have declined in the same
period (from 49.2% in 1970 to 22.1% in 2024, down 27.1% of the total).
Source:
Table 15: Nursing Care Facilities and Continuing Care Retirement
Communities Expenditures; Levels, Percent Change, and Percent
Distribution, by Source of Funds: Selected Calendar Years 1970-2024.
So What? Consumers' liability for nursing home and
CCRC costs has declined by almost half, down 44.9% in the past five
decades while the share paid by Medicaid and Medicare has more than
doubled, up 114.2%.
No wonder people are not as eager to buy LTC
insurance as they would be if they were more at risk for the cost of their
care! No wonder they don't use home equity for LTC when Medicaid
exempts at least $752,000 and in some states up to $1,130,000 of home
equity (as of 1/1/26. The "One
Big Beautiful Bill Act" (OBBBA) set a nationwide limit at $1 million
starting January 1, 2028.) No wonder nursing homes struggle
financially—their dependency on parsimonious government reimbursements is
increasing while their more profitable private payers are disappearing.
Unfortunately, these problems are even worse than the
preceding data suggest. Over half of the so-called "out-of-pocket"
costs reported by CMS are really just contributions toward their cost of
care by people already covered by Medicaid. These are not
out-of-pocket costs in terms of ASSET spend down, but rather only INCOME,
most of which comes from Social Security benefits, another financially
vulnerable government program. Thus, although Medicaid pays a little more
than one-third of the cost of nursing home (and CCRC) care (35.9% of the
dollars in 2024), it covers over two-thirds (67.0%)
of all nursing home patient days.
So What? Medicaid pays in full or subsidizes over
two-thirds of all nursing home patient days. Even if Medicaid pays
nothing, with the entire amount due contributed from the recipient's
income, the nursing home receives Medicaid's dismally low reimbursement
rate.
No wonder the public is not as worried about
nursing home costs as they would be if they were more at risk for the cost
of their care. No wonder nursing homes risk insolvency when so much of
their revenue comes from Medicaid, often at reimbursement rates less than
the cost of providing the care. Consider this for example: “We found that
Medicaid payment rates for the average or median nursing home covered
about 82 cents per every dollar of reported cost nursing homes incurred
caring for Medicaid residents. For approximately 40% of nursing homes,
Medicaid per diem payments covered 80% or less of their estimated per diem
Medicaid costs." (Source: “In
Case You Missed It: New HHS Report Reveals Significant Medicaid Shortfall
For Nursing Homes,” AHCA/NCAL, October 22, 2024)
Private Health Insurance
Don't be fooled by the 8.8% of nursing home costs
that CMS reports as having been paid by "private health insurance" in
2024. That category does not include private long-term care insurance.
(See category definitions
here.) No one knows how much LTC insurance pays toward nursing home
care, because “In most cases, private long-term care insurance reimburses
people for the expenses they pay out-of-pocket and would be classified as
out-of-pocket spending in the NHE data.” (Priya Chidambaram and Alice
Burns, “10
Things About Long-Term Services and Supports (LTSS),” KFF, July 8,
2024) Thus, a large proportion of insurance payments for nursing home care
gets reported as if it were "out-of-pocket" payments. This fact further
inflates the out-of-pocket figure artificially.
Assisted Living
How does all this affect assisted living facilities?
According to the
Genworth Cost of Care Survey for 2024, median ALF cost was $70,800
per year ($5,900 per month), up 1.1% from 2023, but
up 37.2% since 2020. Although assisted living facilities remain mostly
private pay,
almost half of ALFs were “authorized or certified” to participate in
Medicaid and only “a
small minority of state Medicaid programs do not cover services in
assisted living.” Furthermore, “Almost 1 in 5 residents relies
on Medicaid to pay for daily services (18%).” (Find these latter
two quotes under
the source’s “Finance” tab.) Over time, assisted living facilities
have followed nursing homes down the
primrose path of accepting more and more revenue from Medicaid.
Many people who could afford assisted living by
spending down their illiquid wealth, especially home equity, choose
instead to take advantage of Medicaid nursing home benefits. Medicaid
exempts one home and all contiguous property (up to $752,000 or $1,130,000
depending on the state), plus—in unlimited dollar amounts—one
business, one automobile, prepaid burials, term life insurance, household
furnishings, personal belongings and Individual Retirement Accounts not to
mention wealth protected by sophisticated
asset sheltering and divestment techniques marketed by
Medicaid planning attorneys. Income rarely interferes with Medicaid
nursing home eligibility unless such income exceeds the cost of private
nursing home care.
So What? For most people, Medicaid nursing home
benefits are easy to obtain without spending down assets significantly and
Medicaid's income contribution requirement is usually much less expensive
than paying the full cost of assisted living.
No wonder ALFs are struggling to attract enough
private payers to be profitable. No wonder people are not as eager to
buy LTC insurance as they would be if they were more at risk for the cost
of their care. This problem has radically worsened in recent years because
more and more state Medicaid programs are paying for assisted living as
well as nursing home care, which makes Medicaid eligibility more desirable
than ever.
Home Health Care
The situation with home health care financing is very
similar to nursing home financing. According to CMS, America spent $169.4
billion on home health care in 2024, 10.3% more than in 2023 ($153.6).
Medicare (32.9%) and Medicaid (22.5%) paid 55.4% of this total and private
health insurance (not LTC insurance) paid 22.0%. Only 17.9% of home health
care costs were paid out of pocket. The remainder came from several small
public and private financing sources. Data source:
Table 14: Home Health Care Services Expenditures; Levels, Percent Change,
and Percent Distribution, by Source of Funds: Selected Calendar Years
1970-2024.
So What? Only one out of every six dollars spent
on home health care comes out of the pockets of patients and a large
portion of that comes from the income (not assets) of people already on
Medicaid.
No wonder the public does not feel the sense of
urgency about this risk that they would if they were more personally at
risk for the cost of their care.
Other Health, Residential, and Personal Care
This category includes a lot of long-term care
spending that is not encompassed by the nursing home and home health NHE
categories, such as Medicaid home and community based waivers and care
provided in residential care facilities. The trends are very similar.
Americans spent $320.5 billion on these services in 2024, up 9.1% from
$293.7 billion in 2023. Medicare (1.4%) and Medicaid (62.4%) paid 63.8% of
that total; private health insurance and other third parties contributed
31.5%; out-of-pocket expenditures amounted to only 3.5%. Data Source:
Table 13: Other Health, Residential, and Personal Care Services
Expenditures: Levels, Percent Change, and Percent Distribution, by Source
of Funds: Selected Calendar Years 1970-2022
So what? Only one dollar out of $29 spent on these
important LTC services comes out of the pocket of a private payer.
No wonder the public feels so little sense of
worry about planning, saving, investing or insuring for long-term care.
Summary

Source:
National Health Expenditures[2]
Across all three kinds of LTC services
out-of-pocket expenditures account for only $1 in $7.87 spent. Half of
this spending comes from income of people already on Medicaid. Thus only
6.35%, or $1 in $15.74 could have come from spend down of savings.
Bottom line, people only buy insurance against
real financial risk. As long as they can ignore the risk, avoid the
premiums, and get government to pay for their long-term care when and if
such care is needed, they will remain in denial about the need for LTC
insurance. As long as Medicaid and Medicare are paying for a huge
proportion of all nursing home and home health care costs while
out-of-pocket expenditures remain only nominal, nursing homes and home
health agencies will remain starved for financial oxygen.
The solution is simple. Target Medicaid
financing of long-term care to the needy and use the savings to fund
education and tax incentives to encourage the public to plan early to be
able to pay privately for long-term care. For ideas and recommendations on
how to implement this solution, see
www.centerltc.com.
Note especially:
“Better
Long-Term Care for Billions Less,” Cato Institute (2025)
“Medicaid’s
$100 Billion Plus Leak,” Paragon Health Institute (2024)
“Long-Term
Care: The Solution” (2023) with the
Paragon Health Institute at
https://paragoninstitute.org/research-paper-page-moses-ltc-solution-20231002/
“Long-Term
Care: The Problem” (2022) with the
Paragon Health Institute at
https://paragoninstitute.org/long-term-care-the-problem/
“Medicaid
and Long-Term Care” (2020) at
http://www.centerltc.com/pubs/Medicaid_and_Long-Term_Care.pdf
“How
to Fix Long-Term Care Financing” (2017), at
http://www.centerltc.com/pubs/How-To-Fix-Long-Term-Care-Financing.pdf
In the Deficit Reduction Act of 2005, Congress took
some significant steps toward addressing these problems. A cap was placed
for the first time on Medicaid's home equity exemption and several of the
more egregious Medicaid planning abuses were ended. But much more remains
to be done. With the Age Wave cresting and threatening to crash over the
next two decades, we can only hope it isn't too late already.
Stephen A. Moses is president of the Center for
Long-Term Care Reform in Seattle, Washington and a Visiting Fellow with
The Paragon Health Institute. The LTC Center's mission is to ensure
quality long-term care for all Americans. Steve Moses writes, speaks and
consults throughout the United States on long-term care policy. Learn more
at
www.centerltc.com or email
smoses@centerltc.com.
############################
[1] Note
that CMS changed the definition of National Health Expenditure
Accounts (NHEA) categories in 2011, adding for example Continuing Care
Retirement Communities (CCRCs) to Nursing Care Facilities. This change
had the effect of reducing Medicaid's reported contribution to the
cost of nursing home care from over 40% in 2008 to under one-third
(32.8%) in 2009. CMS also created a new category called "Other Third
Party Payers" (7.1%) which includes "worksite health care, other
private revenues, Indian Health Service, workers' compensation,
general assistance, maternal and child health, vocational
rehabilitation, other federal programs, Substance Abuse and Mental
Health Services Administration, other state and local programs, and
school health." For definitions of all NHEA categories, see
http://www.cms.gov/NationalHealthExpendData/downloads/quickref.pdf.
#############################
Updated Wednesday, February 25, 2026,
10:03 AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #26-004: LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Number of hospice providers rises 39.6 percent
between 2019 and 2024, report finds
-
Americans Remain At Elevated Risk Despite Broad
Plan Participation
-
2026 Predictions: LTC Will Be King Again
-
Hidebound scholars harm long-term care
-
Medicaid’s Multiple Roles
-
Washington finalizes long-term care insurance rules
for WA Cares
-
What Happens When the Social Security Trust Fund Is
Exhausted: An Alternative Contingency Policy
-
Poverty and Dependency in the United States,
1939–2023
-
The Current Market For Long-Term Care Planning
-
Medicaid Closes Tax Loophole, Saving Billions for
Taxpayers
-
Low state rates undermine nursing home quality,
especially at Medicaid-reliant for-profits
-
$10,000 a Month for Parents’ Long-Term Care Is a
Growing Crisis—Who Can Afford to Pay?
-
Millions Misspent: How Maine Lost Control of Autism
Medicaid Spending
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Monday, February 23, 2026,
10:03 AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #26-003: LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
The Health Care Cost Curve Is Bending up
Again
-
New tool ultimately could open up senior
living to more people
-
Cleaning Up Medicaid Fraud Will Save
Indiana Millions of Dollars – Governor
-
My Mother Has $260k in an IRA. Is a Nursing
Home Able to Take It?
-
The long term care shake-up: What Unum’s
exit really signals for 2026
-
Low state rates undermine nursing home
quality, especially at Medicaid-reliant for-profits
-
Milliman launches Long-Term Care Index,
providing a benchmark for expected lifetime long-term care costs
-
What Older Americans Want Policymakers To
Know
-
Ross Schriftman Announces Run for Wyoming
House District 37
-
With no way to account for MA pressures,
MedPAC recommends a 4% pay cut for nursing homes
-
How Did We Build a Welfare System that Gave
So Much Money Away?
-
National Health Care Spending Increased 7.2
Percent In 2024 As Utilization Remained Elevated
-
New York’s Per Capita Home Health Aide
Workforce Is Three Times Greater Than Other States’ Average
-
Greater assisted living capacity may delay
nursing home placement for older adults with dementia, study finds
-
US nursing home capacity declines twice as
steep as estimated: JAMA study
-
Minnesota to freeze new Medicaid provider
enrollments in 13 high-risk categories
-
A multi-billion euro shortfall in long-term
care insurance – what critics warned about before its introduction is
now coming to pass
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Monday, January 12, 2026, 10:03 AM (Pacific)
Seattle—
#############################
LTC E-ALERT #26-002: LTC NEWS AND COMMENT
LTC Comment: Do you spend hours searching
the internet for useful articles, key data, and relevant reports to keep
you on the forefront of professional knowledge? Do you lose business
because you’re blindsided by clients or competitors who learn critical
information before you do? Here’s an antidote:
LTC Clippings: The Center for Long-Term
Care Reform notifies subscribers to our LTC Clippings service daily of
information you need to know. Each message contains only the critical
facts about new publications: a title, representative quote, a link to
the original, and our analysis in a sentence or two. To inquire or
subscribe, contact Damon at 206-283-7036 or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC E-Alerts: Once a week, we compile our
daily LTC Clippings into a summary, email it to Center for Long-Term Care
Reform members, and archive it in The Zone, our password-protected
members-only website. Center members also receive our weekly LTC Bullet
op-ed. To join the Center and receive all these benefits and more,
contact Damon at 206-283-7036 or
damon@centerltc.com.
We no longer post our LTC E-Alerts on the
Center’s public access website, but here’s what today’s LTC E-Alert
contained: links, quotes and comments on the following articles, reports,
or data:
-
Pervasive Fraud in Government Health Care Programs
-
‘Far fewer people’ receive institutional services
than HCBS, CMS says
-
Guiding Families Through The Great Wealth Transfer
-
Some Older Adults May Qualify for a New $6,000 Tax
Break
-
Medicaid’s Home Care Support for Family Caregivers
in 2025
-
Retirement Planning Without Kids Demands Attention
to Long-Term Care and Estate Strategies
#############################
"LTC E-Alerts" are
a
feature offered by the Center for Long-Term Care Reform, Inc. to members
at the $150 per year level or higher. We'll track and report to you news
and analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Friday, January 9, 2026, 10:03 AM (Pacific)
Seattle—
#############################
LTC BULLET: HOW REAL IS MEDICAID ASSET SPEND DOWN?
LTC Comment: Does Medicaid asset spend down devastate
everyone who needs long-term care or does it crush the poor, but exempt
the well-to-do? We explore; you decide; after the ***news.***
*** ARGENTINA: Damon and I are about to take a rare
vacation together. There will be a hiatus in our regular bi-weekly LTC
Bullets and weekly LTC E-Alerts, but we will continue to send
our daily LTC Clippings. We’re headed to Bariloche, Argentina from
which we’ll journey by public transportation through Patagonia to Ushuaia,
South America’s southernmost city, then on by ship to Antarctica. In the
meantime, we’ll have full phone and internet connectivity, so keep your
comments and questions coming. The Center for Long-Term Care Reform’s
initiatives on behalf of responsible LTC financing policy will resume
fully upon our return. ***
*** VENEZUELA: Fifty-eight years ago I arrived in
Caracas, Venezuela with thirty fellow Peace Corps volunteers to begin a
two-year stint in an agricultural reform program. Venezuela had
experienced its first ever peaceful, democratic transition of government
only ten years before. Yet it seemed like there were teenagers with
submachine guns on every corner. Rumor (untrue) had it that two PC
volunteers had been shot and killed recently after accidentally running a
police checkpoint. It was like the wild west for this newly minted Poli
Sci BA and my now-late-wife, Judith. We settled in to our site three hours
by bus from Caracas with water we had to boil, electricity only four hours
at night, and little access to groceries beyond bodegas selling beer,
sardines and a hard cheese we were told not to eat. When the Venezuelan
agricultural extensionist and home demonstrator we were supposed to back
up didn’t make an appearance, we improvised, teaching in the elementary
school, working with kids in a 5V club (like 4H), and building furniture
(me) and teaching sewing (Judy). Two kids, Vidal (10 years), now my son’s
middle name, and Dolores, aka “Goofy,” (8 years) hung out at our house
most of the time. Fifty years later, Dolores, who at the time lived in a
mud house, but is now a nun in Colombia, tracked me down on the internet.
We had a reunion a couple years ago in Bogota and we stay in touch. So,
imagine my chagrin watching Venezuela collapse economically over the past
decades causing untold misery for the people in Carmen de Cura, Estado
Aragua, with whom I worked and got to know so well. I hope their long
repression and suffering will end at last with the departure of Maduros
and the death, hopefully, of
Chavismo, although so much remains at risk. Viva Venezuela Libre! ***
LTC BULLET: HOW REAL IS MEDICAID ASSET SPEND DOWN
LTC Comment: How real is Medicaid asset spend down?
It’s a critical question. If, as the conventional wisdom holds, people all
across America are spending down their life’s savings on LTC before they
get any help from Medicaid, we have one kind of problem. It cries out for
even more government money and regulation, the usual appeal.
But if Medicaid asset spend down only crushes the
poor and financially marginal people while giving the middle class and
affluent an asset-spend-down off ramp, as I believe, the problem is
totally different. That suggests we should reconfigure government LTC
spending so it helps the needy first without discouraging everyone else
from planning privately to meet LTC risk.
The Center for Long-Term Care Reform has tackled the
Medicaid asset spend down question many times over the years. See, for
example, most recently, “Understanding
Medicaid Spend Down,” July 12, 2024. Or check out the rest of our 15 “Medicaid
Spend Down Bullets” dating back to June 15, 1999. I summarized the
issue in a paper titled “The
Myth of Medicaid Spend-Down” in 1991. But today, let’s take a fresh
look at the spend down issue.
On December 4, 2025, JAMA Network Open
published “Asset
Spend-Down and Medicaid Enrollment in Nursing Homes,” by Gabriella
Aboulafia, MPP1; Amanda C. Chen, PhD, and David C. Grabowski, PhD. I sent
the following letter to the article’s “corresponding author,” Ms.
Aboulafia. Later I received a thoughtful response from one of the other
authors, the influential, virtually omnipresent scholar, David Grabowski.
I urge you to read the subject article and my letter. Dr. Grabowski’s
feedback and my reply to him may be a topic for another time if he agrees.
In the meantime, here’s my letter. Your comments are welcome.
December 16, 2025
Gabriella Aboulafia, MPP
Corresponding Author
“Asset Spend-Down and Medicaid Enrollment in Nursing Homes”
JAMA Network Open
Dear Dr. Aboulafia,
I am writing in response to your article titled “Asset
Spend-Down and Medicaid Enrollment in Nursing Homes” published
December 4, 2025 in JAMA Network Open.
In that article, you and your co-authors addressed
the issue of nursing home asset spend-down leading to Medicaid
eligibility. You explain that your “main outcome was whether an individual
spent down their assets and became enrolled in Medicaid during their
nursing home stay.” (p. 1/11) You define “spend-down in nursing homes as a
transition from non-Medicaid enrolled to Medicaid enrolled.” (p. 3/11)
You conclude: “Of those who were initially not Medicaid enrolled, 16.4%
spent down their assets during their stay and enrolled in Medicaid ….” (p.
1/11) You infer: “This finding raises concerns both about individuals
impoverishing themselves because of the high cost of care and the
long-term financial sustainability of the Medicaid program.” (p. 1/11)
Although it is not stated explicitly in your article, the clear
implication is that people spend down their assets for private nursing
home or other care before becoming eligible for Medicaid. That is not
necessarily true.
There are many ways for middle class and affluent
people to “transition from non-Medicaid enrolled to Medicaid enrolled”
without expending their assets for long-term care (LTC). While Medicaid
has a very low limit on countable assets, usually $2,000, most large
assets seniors own are exempt, such as home equity, retirement savings, a
vehicle and
many more. Excess countable assets are easily excluded from
consideration by using them to purchase exempt resources as I explain in “Medicaid’s
$100+ Billion Leak.” Besides this simple method of artificial
self-impoverishment, Medicaid planning specialists use special
irrevocable income-only trusts,
Medicaid compliant annuities, and
other legal techniques to qualify much wealthier people for Medicaid.
Your article does mention one method of “shielding assets,” but as you
point out, asset transfers are rare and small compared to the commonplace
practices just described.
You observe that “individuals who once spent their
savings on nursing home care now may deplete their assets in the assisted
living sector and then transition to a nursing home at or near Medicaid
eligibility.” (p. 8/11) That is true, but the same methods people use to
qualify for Medicaid without spending down assets while institutionalized
are equally effective while they remain in the community. In fact,
Medicaid planners routinely advise families to reconfigure their loved
one’s income and assets long before care is needed. They do this not to
ensure Medicaid eligibility upon nursing home admission. Rather, paying
privately for a short time before converting to Medicaid ensures access to
top-quality care. The best nursing homes and home health agencies compete
aggressively for private patients who pay on average 150 percent of the
Medicaid reimbursement rate. By retaining “key money” in this way, middle
class and affluent people lock in access to better nursing homes than poor
and financially borderline individuals, who lack resources to pay
privately for a while, can obtain.
Transition to Medicaid LTC eligibility does not
necessarily involve expending assets for care. The peer-reviewed
literature you cite rarely acknowledges this fact, but the evidence
adduced above establishes it. Assuming transition to Medicaid requires
high private spending leads to unfounded assumptions about ruinous LTC
spending that I rebut in “The
Fallacy of Impoverishment,” “Better
Long-Term Care for Billions Less” and “Long-Term
Care: The Solution.” I respectfully invite you to consider these
points and I would welcome the opportunity to discuss them with you.
Sincerely
Steve Moses
Stephen A. Moses
President, Center for Long-Term Care Reform
smoses@centerltc.com
425-891-3640
#############################
Updated Monday, January 05, 2026,
10:03 AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #26-001: LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
What Medicaid Cuts Could Mean for Home Care
Workers and Family Caregivers
-
Study: Adults in community with dementia at
high risk of being bedbound at life’s end
-
Medicaid Money Laundering Harms Long-Term
Care
-
What you need to know about changes to
Social Security, Medicare and Medicaid in 2026
-
They said it best in long-term care in 2025
-
Retirement Planning Without Kids Means
Focusing On Long-Term Care And Estate Strategies
-
I’m a CEO who’s spent nearly 40 years
talking to presidents, lawmakers and leaders about our long-term care
crisis. They knew this moment was coming
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Monday, December 22, 2025,
10:03 AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-045: LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
‘Spend-down’ rates among nursing home
residents rise with longer stays, study finds
-
Interactive Compendium of LTSS Financing
Options
-
Census Bureau: Americans 55+ comprise
fastest-growing age group of workers in US
-
Long-term-care financing: Some good changes
to WA Cares, new area of recommendation needed
-
Dave Ramsey's Take on Long-Term Care
Planning Is Wrong
-
Better Care for Billions Less: Fixing
Medicaid’s Long-Term Care Incentives
-
The Local Loop: How States Turn Medicaid
into a Government Provider Payday Scheme
-
New Poll: Most Americans Expect Social
Security Benefit Cuts; a Third Believe the Program Won’t Exist When They
Retire
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Friday, December 19, 2025,
10:03 AM (Pacific)
Seattle—
#############################
LTC BULLET: THE
GOLDILOCKS LTC PLAN
LTC Comment: Making
Medicaid pay first would blow the lid off government LTC spending, but
that’s their plan. We explain after the ***news.***
*** ILTCI NEWS from the
2026 conference organizers: “We're thrilled to announce that Jeff Noel, a
30-year Disney leadership veteran and two-time Disney Lifetime Achievement
Award recipient, will take the stage as our keynote speaker,
Sponsored by NGL, at the
2026 ILTCI Conference!” For many more details about this keynoter, go
here. ***
*** MORE about ILTCI:
“Our in-person conference March 8-11, 2026 at the
Rosen Shingle Creek in Orlando, FL is now accepting attendee
registrations! As always, our
agenda will include
numerous educational sessions over two days across
seven tracks with ample time for networking and reconnecting with
colleagues. Everyone who's anyone in Long Term Care Planning will be
there. What about your company? Early Bird Attendee Pricing
available thru Jan 16, 2026!” ***
*** CATO PODCAST with
Center president Steve Moses published:
12/11/2025, “Better
Care for Billions Less: Fixing Medicaid’s Long-Term Care Incentives,”
by Michael Cannon and Stephen Moses, Cato
Quote: “Cato’s
Michael Cannon and the Center for Long-Term Care Reform’s Stephen Moses
examine how Medicaid’s long-term-care eligibility rules let middle- and
upper-middle-class households shelter assets and shift costs onto
taxpayers, driving up spending and lowering quality for the poor. Drawing
on Moses’s new Cato paper
Better Long-Term Care for Billions Less, they explain how perverse
incentives, generous exemptions, and weak estate recovery undermine
private planning and inflate a program already consuming one-third of
Medicaid’s budget.”
LTC Comment:
Click through to the link at the top to hear this 45-minute podcast. Then,
please read the paper and send any questions or comments to
smoses@centerltc.com. To join our mission to fix LTC financing policy
and ensure quality long-term care for all Americans, click
here. To review all of our individual and corporate “Membership Levels
and Benefits,” go
here. Thanks for your support. ***
LTC BULLET: THE
GOLDILOCKS LTC PLAN
LTC Comment: A recent
LTC Discussion Group presentation triggered my interest.
Karen Kopecky, an Economic and Policy Advisor with the Federal Reserve
Bank of Cleveland,
proposed a radical reform
of Medicaid long-term care financing.
Her plan,
co-authored with another economist, involves making Medicaid “primary,”
that is, first payer for long-term care. It’s an intriguing idea. If
Medicaid paid first, consumers would be more likely to buy private LTC
insurance to “top off,” ending “crowd out.” So I contacted Dr. Kopecky. We
had a cordial exchange of views. Here’s my bottom line takeaway. I thank
the
Paragon Health Institute’s
Niklas Kleinworth
for his helpful editing of this piece.
“The Goldilocks LTC
Plan”
by
Stephen A. Moses
Two economists offer an
ingenious proposal to improve long-term care (LTC) financing: make
Medicaid the first payer for services. That is, have it pay before private
LTC insurance so that more people will top off with private coverage.
Their plan rests on a common, but false premise, that LTC causes
widespread ruinous asset spend down leading to Medicaid eligibility. The
plan would be dangerous and expensive if Medicaid financial eligibility is
not tightened substantially first.
In “Welfare-enhancing
public and private insurance arrangements for long-term care risk,”
economists
R. Anton Braun and
Karen A. Kopecky explain the LTC financing challenge like the story of
Goldilocks and the Three Bears. First, they reject two common approaches
to reform. Slashing Medicaid would please taxpayers, but hurt the poor.
That porridge is too cold, morally. Universal LTC coverage would help the
poor, but disadvantage taxpayers. That porridge is too hot, politically.
The authors position their third reform as the happy medium. In their own
words:
Under our reform, benefits continue to be
means-tested, but Medicaid is the primary payer. This third scenario works
best. The poor continue to receive free public insurance, the middle class
top up their Medicaid benefits with private insurance and enjoy higher
welfare and private insurance takeup and profits also increase. (p. 3) …
Making Medicaid the primary payer for LTC insurance while retaining the
means-test increases private LTCI takeup rates, increases the
profitability of insurers, and increases the welfare of low-, middle-, and
high-income individuals. (p. 33)
On its face, this third
concoction seems just right. But there’s a fly in this gruel.
The salutary outcomes
predicted for reform number 3 depend on strictly means testing Medicaid
benefits. Otherwise, everyone would use up Medicaid’s primary benefits and
never get to the point of wanting or needing private insurance. Medicaid
costs would explode and the private LTC insurance market would disappear
entirely.
Thus, we need to know
what these authors believe about means testing Medicaid LTC eligibility
and whether their assumptions are correct. They say Medicaid benefits are
only available to people with very low income and less than $3,000 in
assets. They conclude “most Americans use their savings to pay for formal
long-term care services” leaving “middle-class elderly Americans
particularly exposed to LTC risk.” Consequently, they claim one in ten
Americans incur out-of-pocket (OOP) nursing home expenses of $200,000 or
more.
That clearly expresses
the conventional wisdom about Medicaid spend down. But is it true?
Demonstrably not.
The following table
shows that only 12.9 percent of U.S. LTC expenditures are paid out of
pocket. The vast majority (87.1 percent) come from government programs
(especially Medicaid and Medicare) and other third parties. Furthermore,
half of the out-of-pocket spending comes not from assets, but from
the income people already on Medicaid contribute to offset the
program’s cost for their care. Consequently, only 6.5 percent — or about
$41 billion — of LTC spending could come from asset spend down. That is
too small a portion to support claims that one in ten Americans spend down
their assets at catastrophically high rates.
Table: Out of Pocket
Contributions are a Small Share of Overall LTC Spending
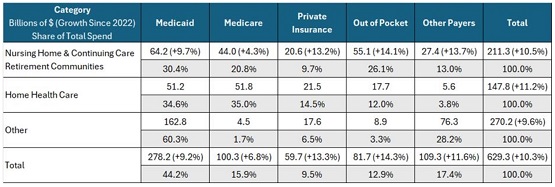
Source: Centers for
Medicare & Medicaid Services,
National Health Expenditures. For definitions of all National Health
Expenditure Accounts (NHEA) categories, see
http://www.cms.gov/NationalHealthExpendData/downloads/quickref.pdf.
Why then do scholars
think out-of-pocket asset spend down is so much higher than the facts bear
out? Faulty estimates based on
statistical micro-simulations are the cause. Ignoring the nonexistence
of evidence, they presume falsely that people must spend down assets
privately for care before qualifying for Medicaid. They run the numbers
through their simulator and voila, catastrophic LTC asset spend down
estimates emerge.
There is a better
explanation of how America spends so much on LTC annually ($629.3
billion), but individual Americans contribute so little ($40.9 billion)
out of pocket. If people with high incomes and assets qualify easily for
Medicaid LTC benefits without spending down, the paradox of high LTC costs
overall combined with low individual asset spend down would be resolved.
Medicaid Income and
Asset Eligibility
High income does not
prevent Medicaid LTC eligibility. Most states subtract private medical and
LTC expenses from income before they apply a low-income standard. Others
cap income but allow special income diversion trusts to achieve the same
outcome. Bottom line: high income people with commensurately high health
care expenses qualify.
Likewise high assets do
not interfere with Medicaid LTC eligibility. Most large assets seniors own
are exempt, including $1 million of home equity and unlimited tax-deferred
retirement savings, a business, a vehicle, and others. Any remaining
countable wealth is easily made exempt by using it to
purchase exempt assets.
The
internet and Medicaid planners offer long lists of exempt assets into
which Medicaid applicants can convert countable resources in order to
become eligible without decreasing their wealth. Mandatory estate recovery
goes largely unenforced so resources protected by Medicaid pass to heirs
further desensitizing future generations to LTC risk and cost.
The Goldilocks LTC
Plan
So, what can we conclude
about the Goldilocks LTC Plan? Make Medicaid primary? That would be a
disaster unless or until Medicaid’s lenient LTC financial eligibility
rules are reformed. But fix that so that people really do have to spend
down their wealth before becoming eligible for Medicaid and the Goldilocks
plan would no longer be needed. If Medicaid truly required impoverishment
to qualify, people would realize the potential financial devastation that
would ensue if they ever needed high-cost long-term care and they would
begin to plan early to save, invest or insure privately for LTC.
If that porridge is too
cold, then try this: keep Medicaid income and asset eligibility limits
generous, but strictly enforce estate recoveries so that eventually all
wealth sheltered in exempt assets is returned to the program to help those
truly in need. That would relieve taxpayers, end Medicaid’s windfall for
heirs, and return dignity to recipients—it isn’t welfare if you pay it
back. It would create a much stronger incentive for all Americans to take
LTC risk and cost seriously in time to prepare.
Real progress toward
resolving long-term care’s many problems will not be made until scholars,
analysts and policymakers set aside the “Fallacy
of Impoverishment” and deal with the reality of Medicaid’s true
impact. The program desensitizes the public to LTC risk and cost leaving
most Americans unprotected and reliant on Medicaid when high LTC costs
occur. That’s fixable with public policy reform that saves money,
eliminates bad incentives, and rewards thoughtful LTC planning. When
worsening budget constraints compel lower LTC spending, drastic change
will become inevitable. Far better to do it now before the fiscal vise
closes narrowing options ever further.
#############################
Updated Monday, December 15, 2025,
10:03 AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-044: LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
The Childfree Care Crisis
-
Medicaid pays 82 cents on the dollar. That hurts
these nursing homes most
-
With inflation, older adults are depleting
retirement savings earlier than expected, survey finds
-
Older adults face high risks of mortality,
institutionalization after hip-fracture surgery, study finds
-
Asset Spend-Down and Medicaid Enrollment in Nursing
Homes
-
BREAKING NEWS: CMS shares updated Medicaid income,
resource standards
-
Medicare Advantage 2026 Spotlight: A First Look at
Plan Offerings
-
Trump said he’s looking into an Australian-style
retirement program for America. Here’s how it works
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Monday, December 8, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC E-ALERT #25-043: LTC NEWS AND COMMENT
LTC Comment: Do you spend hours searching
the internet for useful articles, key data, and relevant reports to keep
you on the forefront of professional knowledge? Do you lose business
because you’re blindsided by clients or competitors who learn critical
information before you do? Here’s an antidote:
LTC Clippings: The Center for Long-Term
Care Reform notifies subscribers to our LTC Clippings service daily of
information you need to know. Each message contains only the critical
facts about new publications: a title, representative quote, a link to
the original, and our analysis in a sentence or two. To inquire or
subscribe, contact Damon at 206-283-7036 or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC E-Alerts: Once a week, we compile our
daily LTC Clippings into a summary, email it to Center for Long-Term Care
Reform members, and archive it in The Zone, our password-protected
members-only website. Center members also receive our weekly LTC Bullet
op-ed. To join the Center and receive all these benefits and more,
contact Damon at 206-283-7036 or
damon@centerltc.com.
We no longer post our LTC E-Alerts on the
Center’s public access website, but here’s what today’s LTC E-Alert
contained: links, quotes and comments on the following articles, reports,
or data:
-
Healthcare gains 33,000 jobs in November
as overall economy sheds 32,000
-
A smaller share of older U.S. adults
live alone today than in 1990
-
Reforming Long-Term Care Policy
-
6 Long-Term Care Rate Increases Hidden
in Winter Renewal Contracts
-
Affordability, Elder Financial Abuse,
and Estate Planning
-
Study Reveals The Age You Hit The
'Tipping Point' Into Frailty
-
5 Key Facts About Medicaid and Provider
Taxes
-
Your Parents' Long-Term Care Could Cost
$10,000 a Month—Who's Really Going to Pay?
-
As pressures mount, so do involuntary
nursing home discharges. Here’s how providers should approach them
-
New AHIP Report Highlights the Vital
Role of Long-Term Care Insurance in Each State
-
7 ESSENTIALS in every Short-Term Care
(Extended Care) & Home Health Care Plan
-
Dangers of Ignoring Long-Term Care
Conversations with Clients
-
Senior Living Satisfaction
-
My Wife and I Planned Our Retirement
Perfectly. Then She Got Sick.
-
OOPS: How the collapse of out-of-pocket
long-term care spending hurts senior living
-
A Look at Waiting Lists for Medicaid
Home- and Community-Based Services from 2016 to 2025
-
Satisfaction with senior living up
despite increasing rates, 2025 J.D. Power study finds
-
Nursing homes singled out in annual
Justice report on elder abuse
-
Medicare Part B Premiums to Jump 9.7% in
2026
-
Family caregivers of people with
Alzheimer’s fail to grasp agitation, survey finds
-
Medicare Advantage enrollment among
long-stay residents grows by more than 180% between 2010 and 2023,
report finds
#############################
"LTC E-Alerts" are
a
feature offered by the Center for Long-Term Care Reform, Inc. to members
at the $150 per year level or higher. We'll track and report to you news
and analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Friday, December 5, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC BULLET: THE
$97 TRILLION LTC PARADOX
LTC Comment: Public
policy incentivizes accumulating wealth, but discourages spending it on
private long-term care (LTC). We explain after the ***news.***
*** REGISTRATION IS
NOW OPEN for the 2026 Intercompany Long Term Care Insurance (ILTCI)
Conference! Organizers report: “Our in-person conference March 8-11,
2026 at the
Rosen Shingle Creek in Orlando, FL is now accepting attendee
registrations! As always, our
agenda will include numerous educational sessions over two days
across
seven tracks with ample time for networking and reconnecting with
colleagues. Everyone who's anyone in Long Term Care Planning will be
there. What about your company? Early Bird Attendee Pricing available
now!” Damon and I will be there to work and cover the
conference, respectively. Register
here. ***
*** MORE ILTCI NEWS:
2026 Session Titles & Descriptions announced. “The wait is over! Our
amazing Program & Education Committee has put together a stellar lineup
of sessions for 2026. These 48 sessions will be scheduled for Monday and
Tuesday of the conference. Click this
link to see the full list, descriptions, and a one page PDF you can
share with your friends and coworkers.” PLUS THIS: Alzheimer's
Association Session Announced. Learn how lifestyle interventions can
reduce the risk of cognitive impairment, how blood-based biomarkers are
enabling earlier, more accessible Alzheimer’s diagnosis and advancements
in treatments. The second half of this session will provide a
comprehensive overview of rapidly moving innovations within dementia
care specialty models including both Medicare and Medicare Advantage
funded approaches. Be sure to add this Wednesday morning session to your
plans!”
*** STC GAINS
ACCEPTANCE as
Dennis Rinner of
GoldenCareUSA explains in
this article that we highlighted in the following LTC Clipping
last week. LTC Clippings are a daily feature we bring to Center
for LTC Reform premium members. Steve Moses tracks the news and analysis
bearing on LTC issues of all kinds. He cites the source, pulls a
representative quote, and gives his interpretation of important
articles, reports, and news items. To join the Center and get access to
our LTC Clippings, LTC Bullets, LTC E-Alerts and
our members-only website, go to
https://centerltc.com/support/index.htm or contact Damon at
206-283-7036 or damon@centerltc.com.
10/30/2025, “7
ESSENTIALS in every Short-Term Care (Extended Care) & Home Health Care
Plan,” by Dennis Rinner, GoldenCareUSA
Quote: “In the
last couple years, there has been a major paradigm shift in the extended
care product space: The landscape is changing. Agents and consumers (in
particular, seniors) are aligned in demanding products that are more
consumer and senior friendly. Everyone wants:
1. Less Underwriting …
2. Less Complicated … 3. Less Costly …Shorter-duration plans can be more
flexible, are significantly lower in cost (more affordable than LTC
alternatives), but they can still be comprehensive in the amount of
coverage clients can select. … Let’s take a closer look at these seven
essentials:
- State
Availability
-
Underwriting
- Unisex
Rates
- Discounts
- Included
Features (Built-In Choices)
- Add-On
Features (Riders)
- Value
Proposition”
LTC Comment:
Click through for all the details in this excellent review of the new
world of extended care coverage. Dennis Rinner has the real world
experience and GoldenCareUSA has the wide reach to support agents and
consumers in the STC and LTC space throughout the country. ***
LTC BULLET: THE $97
TRILLION LTC PARADOX
LTC Comment: Last
January I had this insight. The United States government encourages
Americans to save and invest. Public policy rewards putting money aside
for retirement, building home equity, and amassing life insurance cash
value. But the same government’s policies—ironically and
counterintuitively—discourage spending that accumulated wealth for
high-quality private long-term care. As a result, most Americans who
face elevated LTC expenditures end up on Medicaid, a means-tested public
welfare program. How can that be, I wondered. What are the consequences
for care access and quality? Could different policies make better use of
America’s vast wealth to improve its dysfunctional LTC system?
That puzzle and those
questions led me to draft the following paper. It became the basis for a
vastly revised “Policy
Analysis” titled “Better Long-Term Care for Billions Less,”
published November 13, 2025 by the
Cato Institute. Because the piece published by Cato is very
different from the original draft, focusing mostly on different points,
I want to make the original available to LTC Bullets readers.
Here it is.
“The $97 Trillion LTC
Paradox”
by
Stephen A. Moses
Executive Summary
Government motivates
personal asset accumulation with generous tax incentives. But it
discourages spending the amassed wealth on long-term care (LTC), the
single biggest financial risk aging Americans face. This contradictory
policy undercuts LTC service delivery by relying too heavily on inadequate
public financing. Resolving it in favor of more private LTC financing
would reduce Medicaid expenditures by billions of dollars and
simultaneously expand tax revenues from increased commercial activity.
This paper explains why and how.
Contradictory
Policies
Many government laws and
regulations encourage private wealth accumulation in retirement savings,
home equity, and life insurance. Tax-favored programs like IRAs and
401(k)s reward people for setting aside retirement funds. The federal
government promotes home ownership with subsidized mortgages (FHA, VA,
USDA), mortgage-interest tax deductions, and down payment assistance,
enabling owners to grow equity. Life insurance receives favorable
treatment through tax-deferred growth of cash value and tax-free death
benefits. Thanks to these policies, Americans hold trillions of dollars in
retirement savings ($40T),
home equity ($35T),
and life insurance ($22T),
$97 trillion in total for these resources alone. But little of this
enormous wealth goes to pay for the potentially catastrophic cost of LTC.
How can that be?
LTC includes the
long-term services and supports people require when they cannot perform
basic activities of daily living without assistance. Such assistance may
be needed due to injury, illness, frailty, cognitive impairment or old
age. The need grows exponentially as America’s vulnerable aging population
surges. Most of what we read about LTC in the popular and academic
literature presumes that people all across the country are spending huge
sums of money on nursing homes, assisted living facilities, and long-term
home care. See for example the “Dying
Broke” series by the New York Times and KFF.
The media tell us that many people spend down their life’s savings for
this commonplace, unavoidable and supposedly uncompensated expense. In
truth, the most reliable evidence shows that widespread, ruinous LTC spend
down does not occur. What really happens?
LTC Financing
As the following table
shows, government paid for most of the $629 billion America spent on LTC
in 2023. Medicaid covered 44 percent and Medicare, 16 percent. Private
insurance paid nine percent and other public and private sources, 17
percent. Thus, third parties covered the vast majority of all LTC
expenses, 87 percent. Personal out-of-pocket spending (OOP) accounted for
only 13 percent. As explained below, half of OOP came from income
contributed mandatorily by people already on Medicaid, not from personal
assets. Only six or seven percent of the entire cost of LTC could
possibly come from spend down of private savings. At roughly $40 billion,
out-of-pocket asset spend down barely nicks the tip of the nearly $100
trillion private wealth iceberg.
Source:
National Health Expenditures*
Table: 2023 Total LTC
Spending by Type and Source in Billions of Dollars with the Percentage
Increase Since 2022
* For definitions of
all National Health Expenditure Accounts (NHEA) categories, see
LINK.
How can it be that
private wealth is largely off the table for financing LTC? For one thing,
paid LTC services are far less common than many believe. Fifty-five
percent of people who reach age 65 will not require any paid LTC.
Thirty-one percent will need two years or less.
Those shorter term needs do fall largely on the public, but they are
manageable. Johnson and Wang found that “Nearly nine in ten older adults
have enough resources, including income and wealth, to cover assisted
living expenses for two years.”
It is the remaining 14
percent of paid LTC lasting two years or more, especially the 4 percent
lasting over five years, that incur crushing outlays due to the high cost
of care. Median rates for nursing homes are $320 per day for a private
room and $285 for a semi-private room; assisted living runs $5,350 per
month; homemaker and home health aide services, $30 and $33 per hour,
respectively.
Paid LTC need lasting for long periods at those high rates is clearly
unaffordable by a public largely uninsured privately for the risk. So, as
there is no evidence of widespread catastrophic private LTC spend down, we
must focus on who or what pays instead and how exactly the public avoids
this huge liability.
Medicaid’s LTC
Financing Role
Medicaid pays for most
of the longest, most expensive LTC needs. However, the public welfare
program’s 44 percent share ($278 billion) of total 2023 LTC expenditures
($629 billion) understates its full impact on the service delivery system.
Medicaid recipients are required to contribute most of their personal
income (upwards of half of OOP), including their Social Security benefits
(41% of OOP), to offset Medicaid’s cost for their care.
This supplemental private revenue makes the cost of Medicaid look smaller
and out-of-pocket expenditures appear higher. After co-opting their
private revenue in this way, Medicaid underpays LTC providers, reimbursing
them on average only 70 percent of the rates they would otherwise have
received from private payers.
The combined impact of Medicaid’s commandeering half of total
out-of-pocket LTC spending, approximately $40 billion worth of private
income, and then paying LTC providers often less than the cost of
supplying the care
has had a devastating impact on LTC access and quality. Resulting meager
wages worsen the nationwide shortage of paid caregivers. By dominating LTC
financing while paying sub-market rates, Medicaid also shifts costs to a
dwindling number of private payers who must pay higher rates for their
usually shorter LTC terms of need to compensate.
Thus, Medicaid is the
dominant payer for the longest needs and largest LTC expenditures. But
Medicaid is a public assistance program presumed to have draconian income
and asset limits that block eligibility. That is why most analysts and the
media assume that people must spend down both their income and assets for
LTC until, impoverished, they qualify for Medicaid benefits. It is this
“Fallacy of Impoverishment”
that resolves the paradox of low public out-of-pocket LTC spending despite
sky-high national LTC expenditures.
Financial Eligibility
for Medicaid LTC
Medicaid does require
low income to qualify for LTC benefits, but most state Medicaid programs
deduct private health and LTC expenditures from income before applying the
low-income standard. So, even high income people qualify if their medical
and LTC costs are commensurately high, as they usually are for seniors in
need of expensive, extended care. Some states do cap income instead, but
they allow special income diversion trusts to achieve the same purpose of
enabling higher income people to qualify.
Likewise, high assets do
not interfere with eligibility for Medicaid LTC. Most large assets seniors
own, such as homes, tax-favored retirement savings, or an automobile are
exempt. Countable assets, such as cash, stocks, bonds, really anything
easily convertible to cash, are usually capped at $2,000. But excess
countable wealth is easily converted to exempt status by using it to
purchase exempt assets. See “Medicaid’s $100+ Billion Leak.”
Long lists of exempt resources to facilitate this process are readily
available on line or from financial advisers who specialize in
reconfiguring clients’ income and assets to qualify them for Medicaid LTC
benefits. Bottom line, virtually no amount of income or assets
automatically disqualifies someone from qualifying for LTC funded by
Medicaid and practically any amount of wealth can be reconfigured to
secure Medicaid LTC eligibility.
Mystery Solved
It should be clear now
what is going on. The conundrum of how private out-of-pocket LTC spending
can be so low when total national LTC spending is so high is solved. The
public handles relatively small, shorter-term LTC expenses out of their
available income and assets without severe difficulty. But as LTC need
extends in time and cost, pressure builds on families to find a way to
fund the care. Millions take on the responsibility of caring for loved
ones without pay, but the financial and emotional stress is so great that
many seek help elsewhere. Turned away by Social Security and Medicare,
which do not pay directly for LTC, they eventually discover Medicaid.
There they find the help they seek, but it comes with all the downsides
associated with the program such as the need to rejigger income and assets
to qualify, access and quality problems, institutional bias, long home
care waiting lists, and discrimination due to providers preferring
higher-rate private payers.
Consequences
What are the
ramifications of this unwieldy LTC system for each of its economic
stakeholders? For government, the dominant payer, LTC is a huge
expense that unrelentingly compounds budget deficits and long-term debt.
For the public, LTC is a risk about which they are in denial until
they need it, at which time Medicaid obviates the biggest cost, further
desensitizing future generations to LTC risk. For senior advocates,
LTC means seeking extra government benefits, while missing the irony that
the more government spends on LTC, the less incentive people have to
prepare privately for the risk. For Medicaid planners, LTC
generates big profits from artificially impoverishing affluent clients to
qualify them for benefits while holding back “key money” so their clients
can access the best publicly financed care available to the exclusion of
needier recipients. For care providers, LTC is a race for survival,
as they struggle to supply quality care despite inadequate reimbursement
from public programs that crowd out private payers at market rates. To the
financiers who supply the debt and equity capital to build, operate
and maintain care facilities, LTC requires a constant search to find
profitable projects in a market dominated by poor public payers. Finally,
for insurers, LTC is a hopeless challenge to sell a product
government has been giving away since Medicaid began in 1965. These
players in the LTC marketplace compete to squeeze scraps of benefit or
profit from a centrally planned, government-dominated system that serves
none of them well, and simultaneously defies reform.
Solutions
What can be done? This
entrenched LTC economic system must be disrupted to its core. All payers,
including Medicaid, should pay market rates to all LTC providers. This
would reduce caregiver shortages and mitigate access and quality problems
through market competition. To be able to pay market rates, however,
Medicaid would need to cover fewer recipients. To reduce Medicaid LTC
dependency without harming people in need, the program’s financial
eligibility limits must be tightened gradually so that the public has time
to adjust to a new reality of heightened private LTC risk. To achieve that
objective, the system should exempt everyone under 55 years of age and
anyone already needing LTC from the following changes.
1. Keep Medicaid’s
treatment of income the same, continuing to require a low income standard
after deducting private medical and LTC expenses from total income. Excess
Social Security, pension and other private income should continue to
offset Medicaid’s cost for recipients’ care, but the income flowing to LTC
providers should be at market rates eliminating Medicaid’s artificially
low reimbursements and reinvigorating the entire LTC service delivery
system.
2. Stanch
Medicaid’s $100+ Billion Leak. Stop allowing Medicaid applicants to
purchase exempt assets in order to spend down unlimited, otherwise
countable resources artificially. Instead, treat asset spend down the same
as
income spend down, by limiting it to deductions for actual, documented
private medical or LTC expenditures.
3. Bring seniors’
$14 trillion
of home equity into the LTC financing system by eliminating or vastly
reducing Medicaid’s home equity exemption. At its current 2025 level
between $730,000 and $1,097,000,
Medicaid’s misplaced generosity diverts nearly all home equity away from
LTC funding, enough alone to solve most of LTC’s many access and quality
problems.
4. Stop “Medicaid
Asset Protection Trusts”
and “Medicaid Compliant Annuities”
from diverting vast sums of private wealth from LTC spending into
taxpayer-financed Medicaid expenditures. These legal gimmicks, used
exclusively by the affluent clients of Medicaid planning specialists,
should be illegal.
5. Medicaid’s
5-year asset transfer look-back
is too short to discourage intentional self-impoverishment to qualify for
LTC benefits. Expand it to 20 years. As home ownership and transfers are
publicly recorded by county assessors and recorders, respectively, a
20-year look-back rule could be easily administered. It would end one of
the most commonly recommended early LTC planning methods.
6. End systemic
LTC racism.
Today, affluent Medicaid planners’ clients access the best Medicaid
facilities and services to the exclusion of needier groups, including
racial and socio-economic minorities, by using “key money”
to purchase red-carpet LTC access that the less privileged cannot afford.
When all funders, including Medicaid, pay market rates for care this
unfair advantage benefiting the well-to-do over the underprivileged will
disappear.
7. Give Medicaid
back to the vulnerable aged and disabled people for whom it was originally
intended by reversing the program’s new focus on able-bodied, working-age
adults.
8. Allow states to
experiment with creative ways to do more with less by encouraging and
approving waivers that trade federal matching fund limits for more
state-level LTC policy flexibility.
Implementing these eight
measures will vastly reduce Medicaid LTC caseloads over time, including
the most expensive cases dually eligible for Medicare and Medicaid. The
new program will be better for all who qualify because it will pay market
reimbursement rates adequate to ensure access to and quality of care
across the care continuum from home to nursing home care. Middle class and
affluent people no longer able to qualify for Medicaid LTC while
sheltering wealth will find private pay LTC of higher quality and greater
availability. They will pay market rates instead of higher private rates
inflated by cost shifting caused by earlier artificially low Medicaid
rates. With enormous sums of new private financing flowing through the LTC
service delivery system at market rates, commercial activity will flourish
generating additional tax revenue as more caregivers and LTC providers
join the newly profitable sector.
Obstacles
This is an attractive
picture. But getting from the dysfunctional system we have now to this
vastly different organization of incentives and results is a problem.
Critics will excoriate this new approach as uncaring toward people in need
despite the irony that most of them believe incorrectly that the existing
LTC system already impoverishes millions. But in truth this change will
mean better LTC for those most in need who will continue to qualify for
assistance from Medicaid. Others who become responsible to pay for their
own LTC before they qualify for Medicaid will have time to adjust and
prepare before they are affected. People already in need of LTC or under
age 55 will remain unaffected and covered by Medicaid.
The biggest challenge to
re-inventing LTC in this way is how to awaken the public to the new
reality without inciting opposition. No longer will people be able to
ignore the risk and cost of LTC in their younger years and still receive
Medicaid LTC in old age while preserving wealth. How to achieve a
transition from current LTC complacency and government dependency to
serious personal responsibility and planning is the major obstacle.
Families struggling to make ends meet and save for their own retirement
will not look kindly at a new obligation to save, invest or insure for LTC.
How can they be relieved of that burden while simultaneously reducing the
public financing option that has failed everyone so miserably?
Answers
The solution is to
re-prioritize LTC among life’s responsibilities. As this paper has
explained, public policy rewards the accumulation of savings, but
discourages the use of private wealth to fund LTC. Why should amassing
wealth that will pass to heirs if unspent take precedence over funding
quality LTC for the living? Why should Medicaid incentivize heirs to use
welfare-financed care for their infirm parents’ LTC needs? What if public
policy prioritized preparing privately for future LTC need instead? What
might such policy look like?
Step one is to inform
the public about the loss of Medicaid as a late-life wealth preserving
safety net for the middle class and affluent. Then establish and
promulgate new LTC planning goals for consumers to achieve no later than
age 65 as a precondition for any later Medicaid help with catastrophic
costs. Give every citizen an objective analysis of their LTC risk and an
estimate of the likely cost of the care they may need some day. Each
person could then know what they need to set aside to cover their average
expected LTC need. Research shows that an overall average is $70,000
invested by age 65 will cover median paid LTC need.
Of course individuals may need to set aside less or more depending on
their unique circumstances. While ensuring that every individual’s average
LTC risk is covered by private funding would not eliminate Medicaid’s back
end catastrophic risk, it would substantially reduce that risk enabling
Medicaid to do a better job for all remaining long-duration recipients.
How can people achieve
their needed level of LTC savings without undue pressure on their ongoing
living needs? One way could be to allow or require individuals and
families to earmark other resources they are accumulating, such as
retirement savings, home equity or life insurance, to be used for LTC if
and only if otherwise unaffordable LTC needs occur in the future. In that
manner, wealth being accumulated with strong public policy inducements can
be repurposed to fund future LTC without impairing families’ current cash
flow. Savings that would otherwise pass through inheritance would go to
fund higher quality LTC for the living and create a stronger inducement
for younger generations to save, invest or insure for their own future LTC
need.
Conclusion
Some government policies
encourage citizens to accumulate vast savings. But other public policies
discourage them from spending this wealth on LTC. Easy access to Medicaid
LTC benefits late in life enables people to ignore LTC risk and cost when
they are young without drastic financial consequences later. As a result,
few people plan, save, invest or insure for LTC early in life and they end
up dependent on Medicaid late in life. But Medicaid distorts the LTC
market by dominating it, paying too little for care, and thus causing
caregiver shortages and other access and quality problems.
To fix LTC, all payers,
including Medicaid, should pay market rates enabling competition to
ameliorate service delivery and financing problems. For Medicaid to pay
market rates, however, LTC caseloads must decline dramatically. To reduce
LTC caseloads, tighten Medicaid LTC financial eligibility limits by
ensuring that recipients actually spend down income and assets for real
private medical and LTC expenses before becoming eligible. To prepare the
general public for this less easily available Medicaid LTC program,
identify each person’s likely LTC risk and cost, then let them earmark
enough from assets they are otherwise accumulating to satisfy their LTC
planning responsibility if and only if needed to fund their future LTC.
This arrangement will
induce people to plan for LTC earlier and to pay privately for their care
when needed. That private spending will reduce the cost of LTC for
Medicaid. Medicaid, relieved of covering so many people who should, could
and would have paid for their own LTC absent current public policy
incentives to the contrary, will be able to do a better job for all
remaining, genuinely needy recipients. The terrible condition of LTC
service delivery and financing in the United States is not the result of
too little government funding and regulation, but too much. Reconfiguring
the carrots and sticks in public policy to redirect vast personal savings
toward private LTC financing is the key to improve LTC for everyone, rich
and poor alike.
#############################
Updated
Friday, November 21, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC BULLET: CATO ON LTC
LTC Comment: Cato published papers on long-term care
financing reform in 2005 and again this year. After slow progress for two
decades a change for the better may be coming soon. Reflections after the
***news.***
*** REGISTRATION IS NOW OPEN for the 2026
Intercompany Long Term Care Insurance Conference! Organizers report: “Our
in-person conference March 8-11, 2026 at the
Rosen Shingle Creek in Orlando, FL is now accepting attendee
registrations! As always, our
agenda will include numerous educational sessions over two days across
seven tracks with ample time for networking and reconnecting with
colleagues. We still have room for
exhibitors and
sponsors! Please contact us at
info@iltciconf.org if you are interested in either opportunity to
showcase your products and services to our attendees. Everyone who's
anyone in Long Term Care Planning will be there. What about your company?”
Damon and I will be there to work and cover the conference, respectively.
See you then. ***
LTC BULLET: CATO ON LTC
LTC Comment: In 2005, public policy regarding LTC
financing was in ferment. The U.S. economy slowed to a crawl. State and
federal politicians worried about making fiscal ends meet. Medicaid LTC
expenditures soared while public interest in private LTC insurance waned.
Policymakers worried about funding LTC, but frequent appeals for a big new
entitlement program for that purpose fell flat. The best thing I can say
about that time two decades ago is that LTC and fiscal responsibility
still mattered to legislators and policymakers.
I spent half that year commuting from Seattle to
Washington, DC—2 weeks on, 2 weeks off—to advocate for tighter Medicaid
financial eligibility rules, stronger estate recoveries, and more support
for private LTC insurance. I spoke to everyone who would listen from all
the LTC trade associations, to members of Congress and their staffs, to
experts at the most influential think tanks, Cato, AEI, and Heritage. We
had high hopes to pass legislation that would encourage the public to plan
early for LTC and save, invest or insure for that risk instead of ending
up on Medicaid by default.
That was how things stood on September 1, 2005 when
the Cato Institute published “Aging
America’s Achilles’ Heel: Medicaid Long-Term Care.” If you don’t feel
like reading that 18-page article, listen instead to
this 6-minute interview that summarizes it generated by
Google Illuminate. Or, better yet, check out
this hour-long debate between yours truly and Vincent Russo, who is a
Medicaid planner with three offices in New York as well as a founding
member and fifth president of the National Academy of Elder Law Attorneys,
the Medicaid planners’ trade association.
As it turned out, we did get meaningful legislation
the following March 2006 when Vice President Dick Cheney flew back from
the Middle East expressly to break a Senate deadlock and pass the Deficit
Reduction Act of 2005. The
DRA ’05 enacted the first ever cap on Medicaid home equity, setting
the exemption between $500,000 and $750,000 at state option. The
legislation also unleashed the LTC Partnership program that had been
stifled for years by a prohibition against exempting sheltered assets from
estate recovery. Those were two steps in the right direction, but not
nearly enough.
Unfortunately, the DRA ’05 was the last significant
progress America has made toward saving Medicaid LTC benefits for the
needy and diverting middle class and affluent people toward savings,
investment or insurance for LTC. An amazing thing happened in the U.S.
during those intervening years. The Federal Reserve pushed interest rates
to near zero setting off a government, corporate, and personal spending
spree such as the country had never seen before. State and federal budgets
exploded; national debt soared to $38 trillion; and personal wealth from
home equity, stocks, and bonds skyrocketed. The wealthy profited more than
ever; the needy made few if any gains.
As long as this economic party continued, the
powers-that-be had little interest in fixing Medicaid LTC. I’d noticed
over the years that when the economy went into recession and politicians
couldn’t stay within budgets, they showed interest in ideas and
recommendations to control Medicaid LTC costs, especially when proposed to
improve care access and quality at the same time. But when the good times
rolled, they lost interest. That’s why I’m hopeful now.
The U.S. economy is showing signs of stress. Interest
rates are up. National debt is in the stratosphere. Interest on the debt
exceeds defense expenditures. Deficits approaching $2 trillion per year
increase the debt immediately and boost debt-service costs over time.
Doubts emerge that the United States can service its debt going forward.
That means it will struggle repaying bondholders for their investments
resulting in America’s creditors losing confidence in the dollar. The
“debasement trade” tempts investors to abandon fiat currencies like
the dollar for hard assets like gold and silver.
In other words, conditions are lining up for
policymakers and politicians to take the need for LTC financing reform
seriously again. Therefore, timing was right for another Cato paper to
point the way. Cato published “Better
Long-Term Care for Billions Less” on November 13, 2025, bookending its
2005 coverage of the issue. Please read the new paper or listen to
this 7-minute “interview” summarizing it. Then share your feedback,
positive or negative, with me at
smoses@centerltc.com. Thanks for your time and consideration.
#############################
Updated
Monday, November 17, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC E-ALERT #25-042: LTC NEWS AND COMMENT
LTC Comment: Do you spend hours searching
the internet for useful articles, key data, and relevant reports to keep
you on the forefront of professional knowledge? Do you lose business
because you’re blindsided by clients or competitors who learn critical
information before you do? Here’s an antidote:
LTC Clippings: The Center for Long-Term
Care Reform notifies subscribers to our LTC Clippings service daily of
information you need to know. Each message contains only the critical
facts about new publications: a title, representative quote, a link to
the original, and our analysis in a sentence or two. To inquire or
subscribe, contact Damon at 206-283-7036 or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC E-Alerts: Once a week, we compile our
daily LTC Clippings into a summary, email it to Center for Long-Term Care
Reform members, and archive it in The Zone, our password-protected
members-only website. Center members also receive our weekly LTC Bullet
op-ed. To join the Center and receive all these benefits and more,
contact Damon at 206-283-7036 or
damon@centerltc.com.
We no longer post our LTC E-Alerts on the
Center’s public access website, but here’s what today’s LTC E-Alert
contained: links, quotes and comments on the following articles, reports,
or data:
-
New Paper: Better Long-Term Care for Billions Less
-
Better Long-Term Care for Billions Less
-
Long-term care is ‘elephant in room’ in financial
planning discussions, despite concerns
-
Better than Boca
-
The cost of care is gutting the American dream.
Here's how to fix it.
-
Robots will play a growing role in elder care,
experts say
-
Genworth Plans to Offer Market-Linked Long-Term
Care Benefits
-
Number of ‘solo-agers’ skyrockets, AARP survey
finds
-
I just retired with a cushy $2M nest egg but my
wife, 62, has been diagnosed with a serious illness and may need
long-term care. What do we do now?
#############################
"LTC E-Alerts" are
a
feature offered by the Center for Long-Term Care Reform, Inc. to members
at the $150 per year level or higher. We'll track and report to you news
and analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Monday, November 10, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC E-ALERT #25-041: LTC NEWS AND COMMENT
LTC Comment: Do you spend hours searching
the internet for useful articles, key data, and relevant reports to keep
you on the forefront of professional knowledge? Do you lose business
because you’re blindsided by clients or competitors who learn critical
information before you do? Here’s an antidote:
LTC Clippings: The Center for Long-Term
Care Reform notifies subscribers to our LTC Clippings service daily of
information you need to know. Each message contains only the critical
facts about new publications: a title, representative quote, a link to
the original, and our analysis in a sentence or two. To inquire or
subscribe, contact Damon at 206-283-7036 or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC E-Alerts: Once a week, we compile our
daily LTC Clippings into a summary, email it to Center for Long-Term Care
Reform members, and archive it in The Zone, our password-protected
members-only website. Center members also receive our weekly LTC Bullet
op-ed. To join the Center and receive all these benefits and more,
contact Damon at 206-283-7036 or
damon@centerltc.com.
We no longer post our LTC E-Alerts on the
Center’s public access website, but here’s what today’s LTC E-Alert
contained: links, quotes and comments on the following articles, reports,
or data:
-
Rise in premature deaths prevents Americans from
reaching age of Medicare eligibility, study finds
-
Layin’ It on the Line: The long-term care crisis
2.0 — Why the government may force you to buy coverage
-
Measure to allow investment of WA Cares tax dollars
in stock market on track for approval
-
Are taxpayers wasting $86 billion on SilverSneakers
and Medicare Advantage goodies they don't use?
-
Long-term services: Lots of ideas but who will pay
for them?
-
Medicaid payment pause could have unintended
consequences for assisted living providers, residents
-
As Pickleball Continues to Gain Players, Injuries
Are Increasing
#############################
"LTC E-Alerts" are
a
feature offered by the Center for Long-Term Care Reform, Inc. to members
at the $150 per year level or higher. We'll track and report to you news
and analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Friday, November 7, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC BULLET: OOPS! THE COLLAPSE OF OUT-OF-POCKET
LONG-TERM CARE SPENDING AND ITS CONSEQUENCES
LTC Comment: Academics and the media claim millions
of middle class Americans are spending their life’s savings on long-term
care until they’re broke. We examine this “Fallacy
of Impoverishment” after the ***news.***
|
*** TODAY'S LTC BULLET is sponsored by Claude
Thau (BackNine Insurance). BackNine gives you a free
personalized website at no cost. Your clients (& family & friends)
can, with as little or as much of your involvement as you or they
want, buy life insurance and LTCi, and can speed issue by scheduling a
paramed and uploading medical records immediately. We quote
stand-alone LTCi, linked-benefit and life with a LTC rider
side-by-side. Claude is the lead author of Milliman’s annual Broker
World LTCi Survey & a past Chair of the Center for Long-Term Care
Financing. Contact him at 913-707-8863 or
claude@back9ins.com to learn about more
great BackNine features and services. *** |
*** REGISTRATION IS NOW OPEN for the 2026
Intercompany Long Term Care Insurance Conference! Organizers report: “Our
in-person conference March 8-11, 2026 at the
Rosen Shingle Creek in Orlando, FL is now accepting attendee
registrations! As always, our
agenda will include numerous educational sessions over two days across
seven tracks with ample time for networking and reconnecting with
colleagues. We still have room for
exhibitors and
sponsors! Please contact us at
info@iltciconf.org if you are interested in either opportunity to
showcase your products and services to our attendees. Everyone who's
anyone in Long Term Care Planning will be there. What about your company?”
Damon and I will be there to work and cover the conference, respectively.
See you then. ***
*** BOLO. The
Cato Institute plans to publish
Steve Moses’s “Policy Analysis” titled “Better Long-Term Care for
Billions Less” on November 11. This new paper reveals why America’s LTC
service delivery and financing systems are such a mess. It proposes a
creative new approach to resolve all LTC’s problems. Be on the lookout.
***
LTC BULLET: OOPS! THE COLLAPSE OF OUT-OF-POCKET
LONG-TERM CARE SPENDING AND ITS CONSEQUENCES
LTC Comment:
Anecdotes abound that some people spend enormous sums on long-term
care (LTC). What is lacking is any evidence that catastrophic LTC asset
spend down is widespread. The evidence we do have is all to the contrary.
For example, consider the following decade-by-decade tables derived from
annual
National Health Expenditure data. Start with the most recent year for
which we have data, 2023. It shows that overall out-of-pocket LTC spending
for nursing homes, continuing care retirement communities, home health
care and other health, residential, and personal care is only 12.9%. What
can we make of this?
Source:
National Health Expenditures*
“Other” includes “health, residential, and personal care”
* For definitions of all National Health Expenditure Accounts (NHEA)
categories, see
http://www.cms.gov/NationalHealthExpendData/downloads/quickref.pdf.
If you didn’t have these facts right in front of you,
what percentage of U.S. spending for LTC would you guess that people pay
out of pocket? You’ve heard Medicaid requires impoverishment, so that
implies a lot of private spending. You know LTC insurance is unpopular,
owned by only 3.1% of Americans, so that source wouldn’t contribute
much. Everyone says Medicare doesn’t pay for LTC, so no help there. The
other public and private third-party LTC payers are each relatively small
and not well known. So, you could be excused for guessing that
out-of-pocket LTC expenditures must be half, maybe even two-thirds of
total LTC spending.
Actually, that guess wouldn’t be far off from what
peer-reviewed scholars have estimated over the years.
Kemper, Komisar, and Alecxih claimed in 2005 that 45% of LTC
expenditures were “uninsured private expense.” In 2016,
Favreault and Dey said: “Families will pay about half of the costs
themselves out-of-pocket.”
Favreault and Johnson reckoned in 2021 that “out-of-pocket payments”
were 57% of “total LTSS expenditures.” The following NHE tables, covering
2020, 2010, and 2000, reveal that actual OOP spending during those periods
was 12.0%, 14.1% and 19.9%, respectively. How could respected scholars get
such an important statistic so wrong? And why?
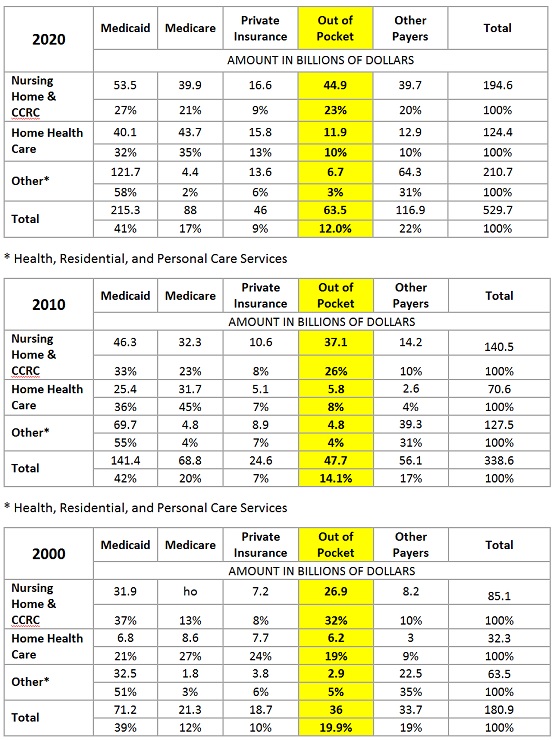
How and Why Do Scholars Estimate OOPS at Double or
Triple the Actual Rate?
Instead of using the actual NHE data provided by CMS
that I’m citing here, scholars chose to rely on “micro simulations”
generated by software like the Urban Institute’s “Dynamic
Simulation of Income Model (DYNASIM).” Here’s how DYNASIM describes
its seductive capabilities:
Using the best and most recent data
available, [DYNASIM] projects the size and characteristics—such as income
and health status—of the US population for the next 75 years. DYNASIM can
also describe “what if” scenarios, showing how outcomes would likely
evolve under changes to public policies, business practices, or individual
behaviors. With this model, we can show how different groups will fare
over time, who is moving ahead and who is being left behind, and which
groups would win and lose under various policy options.
In other words, as it applies to our current
question, if you plug in Medicaid’s financial eligibility rules, DYNASIM
will grind out a statistic for how much people must have had to pay
out-of-pocket for LTC based on national data for how much income and
wealth the public starts with before they confront LTC costs. On top of
that, DYNASIM points scholars and policymakers toward who “would win and
lose under various policy options.” Scholars like simulations based on
assuming LTC causes impoverishment because they “point” to the policy
options most academics prefer, i.e., more public, less private financing.
What’s Wrong with DYNASIMulation?
So, exactly how do the experts come up with those
high OOP spending estimates? First, they cite sources that say Medicaid
LTC eligibility depends on having “low income,” only $967 per month and
low assets, usually $2,000. These are the Supplemental Security Income (SSI)
limits that do guarantee Medicaid eligibility once reached. Then they
assume everyone spends down any excess wealth they possess for private LTC
until they reach those levels and become eligible for Medicaid. Their
simulator applies those strict financial eligibility criteria to national
income and wealth data and conclude that half or more of all LTC
expenditures must come from private out-of-pocket spending. QED.
What’s wrong with this method? Why does it produce
estimates that are three or four times what the actual data show? Although
people who fall within those low Medicaid income and asset limits do
qualify for LTC benefits, that does not mean that other people with
substantially more income and assets cannot qualify nor that they must
spend down their savings for private LTC before becoming eligible for
Medicaid.
People with high incomes qualify because in most
states Medicaid deducts their private health care spending from their
incomes before applying a low income standard. Some states do apply an
income cap, but they allow special income diversion trusts to achieve the
same purpose. Either way, high income people qualify easily for Medicaid
LTC benefits.
Nor do high assets disqualify people from Medicaid
LTC. Most large assets seniors own are exempt for determining eligibility.
Exempt assets include most home equity, home improvements, IRAs, a side
business, a vehicle, prepaid funeral expenses, all personal belongings and
household furnishings and others, lists of which are available
online and from
Medicaid planners. Extra countable assets people own are easily made
exempt by using them to purchase resources that are exempt, thus achieving
eligibility while preserving wealth in a different form. This is “Medicaid’s
$100+ Billion Leak.”
In other words, Medicaid LTC financial eligibility is
more complicated than simply applying the presumed income limit of $967
per month and the $2,000 cap on countable assets to national income and
asset ownership data. That simple-minded simulation produces vastly
over-estimated numbers for OOPS. So, given that CMS provides hard data
every year on actual OOP spending, we need to ask not only how the experts
come up with such inflated estimates, but why they do it.
I think the reason scholars inflate OOPS is the
ideological proclivity among academics toward “LTC solutions” that involve
more government spending and regulation. Most of their articles, reports
and books that estimate very high OOP spending then conclude that to
relieve the awful burden of LTC on families, the only viable solution is
to increase Medicaid spending, add LTC to Medicare, or concoct a new
compulsory, payroll-funded, LTC entitlement on the model of Social
Security and Medicare.
But all such proposals have fallen flat. The time for
big government entitlement programs has passed. We’re likely to lose the
ones we already have before a new one for LTC comes along. The national
debt exceeds
$38 trillion. Spending surpasses revenue this year by $1.8 trillion.
We’re on the brink of being unable to service the national debt, which
means the bond market may demand austerity, not a promising economic
environment for big new government spending programs going forward.
Consequences of Declining OOPS
Consider the history of actual OOPS spending over the
years. Here are the remaining tables for each start of decade since 1970.
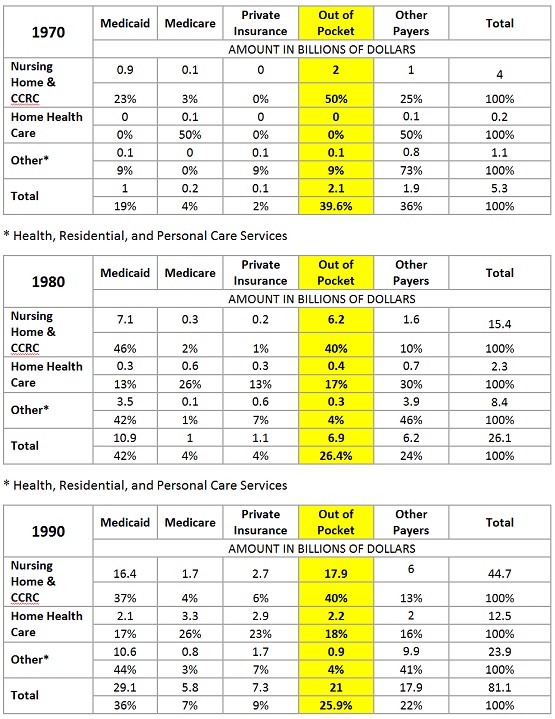
Note the gradual decline in OOPS starting from almost
40% in 1970, only five years after Medicaid began subsidizing LTC with
virtually unlimited federal matching funds, to 25.9% in 1990, finally
dropping by half again to 12.9% in 2023. Clearly the burden of
out-of-pocket LTC spending on the public has declined radically over the
years.
These facts have consequences. The decline in OOPS
explains why most Americans do not worry about LTC until they need it. As
their LTC spending soars, they easily qualify for Medicaid. The next
generation receives that message when, thanks to Medicaid, their
inheritances are unencumbered by their parents’ LTC costs. The cycle is
perpetuated as each new generation fails to save, invest or insure for LTC
and ends up relying on Medicaid.
Today, Medicaid is the dominant payer for all forms
of LTC, 44.2%. In 2023, as the first table above shows, it covered, 30.4%
of nursing home care, 34.6% of home health care, and 60.3% of “other”
health, residential, and personal care services. Medicaid pays nursing
homes and other LTC providers dismally low reimbursements, often less than
the cost of providing the care. Much higher private-pay revenue for
nursing homes has collapsed to only 7%. High dependency on low Medicaid
reimbursements is the cause of LTC’s biggest problems including caregiver
shortages, poor access and low quality.
What to Do Instead
Instead of fantasizing catastrophic LTC spending,
based on wishful simulations, to scare up demand for a big new,
compulsory, payroll-funded LTC entitlement program, here’s what needs to
happen instead.
Recognize that OOPS is much lower than the scare
mongers claim. Strengthen Medicaid financial eligibility rules so they do
not allow middle-class and affluent people to qualify for LTC benefits
while preserving wealth and without spending down for their own care. Save
and improve Medicaid as a LTC safety net for the genuinely needy who
currently receive the program’s worst facilities and services.
For full documentation of these problems and detailed
proposals to solve them, see the
Paragon Health Institute’s “Long-Term
Care: The Problem” and “Long-Term
Care: The Solution.” Watch for the
Cato Institute’s “Better Long-Term Care for Billions Less,”
forthcoming November 11.
#############################
Updated
Monday, November 3, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC E-ALERT #25-040: LTC NEWS AND COMMENT
LTC Comment: Do you spend hours searching
the internet for useful articles, key data, and relevant reports to keep
you on the forefront of professional knowledge? Do you lose business
because you’re blindsided by clients or competitors who learn critical
information before you do? Here’s an antidote:
LTC Clippings: The Center for Long-Term
Care Reform notifies subscribers to our LTC Clippings service daily of
information you need to know. Each message contains only the critical
facts about new publications: a title, representative quote, a link to
the original, and our analysis in a sentence or two. To inquire or
subscribe, contact Damon at 206-283-7036 or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC E-Alerts: Once a week, we compile our
daily LTC Clippings into a summary, email it to Center for Long-Term Care
Reform members, and archive it in The Zone, our password-protected
members-only website. Center members also receive our weekly LTC Bullet
op-ed. To join the Center and receive all these benefits and more,
contact Damon at 206-283-7036 or
damon@centerltc.com.
We no longer post our LTC E-Alerts on the
Center’s public access website, but here’s what today’s LTC E-Alert
contained: links, quotes and comments on the following articles, reports,
or data:
-
Are Consumers Ready For The Great Wealth Transfer?
-
Who Will Care For Aging Clients?
-
Gen X could be ‘most financially vulnerable cohort’
facing retirement: report
-
Fiscal sanity or risky gamble? Allowing state to
invest WA Cares Fund in stock market
-
New report finds wide variation across states in
financial strain among family caregivers
-
New Research on Long-Term Care Insurance
Partnerships
-
90% of Americans plan to skip the No. 1 piece of
Social Security advice, study finds
-
My husband and I have $7K in Social Security and
$2.5 million in stocks. What could go wrong?
-
9 Things Retirees Should Stop Buying, According to
Financial Experts
#############################
"LTC E-Alerts" are
a
feature offered by the Center for Long-Term Care Reform, Inc. to members
at the $150 per year level or higher. We'll track and report to you news
and analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Monday, October 27, 2025,
10:03 AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-039: LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Deciding on Senior Living? 10 Things You Should
Know
-
8 Insurance Benefits You Lose After 70
-
Shutdown or not, there are things to do
-
Exposure to bright lights at night linked to
increased risk of heart disease, study finds
-
Investment Firm Acquires LifeSecure From Michigan
Blue
-
LTCi makes a difference in family caregiving, study
finds
-
Nationwide expands hybrid long-term care lineup
with new annuity option
-
Strengthening a safety net requires reforms to
long-term care through Medicaid
-
Morgan Stanley: Longevity Is Redefining Financial
Planning
-
Pushed from liberal-leaning states, home care
providers may eye expansion in Arizona, Florida, Texas, attorney says
-
The Top 5 Reasons For Turmoil In The Medicare
Advantage Market
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Friday, October 24, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC BULLET: A BETTER LTC ANSWER THAN WA CARES
LTC Comment: As
WA Cares slides down the slippery fiscal slope facing all compulsory,
payroll-funded government entitlements, we bring you a better option,
after the ***news.***
*** REGISTRATION IS NOW OPEN for the 2026
Intercompany Long Term Care Insurance Conference! Organizers report: “Our
in-person conference March 8-11, 2026 at the
Rosen Shingle Creek in Orlando, FL is now accepting attendee
registrations! As always, our
agenda will include numerous educational sessions over two days across
seven tracks with ample time for networking and reconnecting with
colleagues. We still have room for
exhibitors and
sponsors! Please contact us at
info@iltciconf.org if you are interested in either opportunity to
showcase your products and services to our attendees. Everyone who's
anyone in Long Term Care Planning will be there. What about your company?”
Damon and I will be there to work and cover the conference, respectively.
See you then. ***
*** LTC CLIPPINGS are a daily feature we bring to
Center for LTC Reform premium members. Steve Moses tracks the news and
analysis bearing on LTC issues of all kinds. He cites the source, pulls a
representative quote, and gives his interpretation of important articles,
reports, and news items. To join the Center and get access to our LTC
Clippings, LTC Bullets, LTC E-Alerts and our
members-only website, go to
https://centerltc.com/support/index.htm or contact Damon at
206-283-7036 or damon@centerltc.com. In the meantime, here’s a sample
LTC Clipping highlighting an article by today’s Guest LTC Bullet
author Elizabeth New.
7/16/2025, “Estate
recovery is fair — if Medicaid is for the needy,” by Elizabeth New,
Washington Policy Center
Quote: “The American Medical Association (AMA)
recently voted
to oppose a federal
requirement that says states must seek to recover long-term care (LTC)
Medicaid costs from the estates of deceased beneficiaries. That’s bad
advice from the AMA and implies that states are doing a good job with
estate recovery efforts. They’re not. … Stephen Moses, a longtime advocate
of estate recovery and president of the Center
for Long-Term Care Reform, has argued for years that strong recovery
policies promote personal responsibility and discourage Medicaid gaming.
He’s right. Pretending that all estate recovery is punitive or unjust
ignores the fact that the real injustice lies in allowing people with
means to use a safety net they do not need. The AMA's vote of opposition
sends the wrong message, and lawmakers just missed a cost-saving beat in
their big bill. Medicaid is not an inheritance-preservation program. It is
a last-resort lifeline. Federal and state lawmakers should not be shamed
for treating it that way.”
LTC Comment: Hearty thanks to Elizabeth New of
the Washington Policy Center for this spot-on article. She is a tireless
advocate for sensible LTC financing policy. For more on the topic, read my
1988 study for the USDHHS Inspector General titled “Medicaid
Estate Recoveries.” Most of its recommendations, including mandatory
estate recoveries, became federal law in the Omnibus Budget Reconciliation
Act of 1993. ***
LTC BULLET: A BETTER SOLUTION FOR WASHINGTON THAN WA
CARES
LTC Comment:
Elizabeth New, nee Hovde (her former byline) is Director of the Center
for Health Care and Center for Worker Rights at the
Washington Policy Center, a free market oriented think tank in
Washington State. We’ve cited her analysis and criticism of WA Cares in
LTC Clippings at least six times in the past year. She indicts
Washington State’s LTC entitlement program as insufficient, mismanaged,
and unfairly structured, placing an undue burden on taxpayers. Today Ms.
New brings us a broader perspective on her thinking about Medicaid’s and
WA Cares’ roles in long-term care service delivery and financing. Here’s
how she introduces today’s LTC Guest Bullet:
Elizabeth New: A funny thing happened on the
way to WA Cares.
As I studied Washington state’s new, mandatory
long-term care program — which distorted the private insurance market, has
solvency issues, will offer limited help to only some workers and taxes
low-income earners to subsidize those with no need for public aid — I
learned about the even more concerning burden Medicaid Long-Term Care is
placing on taxpayers.
The following policy paper, written for Washington
state lawmakers, is the result of that deeper investigation. It proposes
reforms to Medicaid Long-Term Care that can preserve the safety net for
people in true need, while protecting taxpayers from a program that has
been stretched beyond its design.
My analysis draws on key insights from industry
experts, including the foundational work of Stephen Moses. I invite you to
read, “Strengthening
a safety net requires reforms to long-term care through Medicaid.”
Introduction
Washingtonians are living longer. More people are —
and will end up — using long-term-care services to help them with
activities of daily life.
Some people need financial help with long-term care,
which state and federal taxpayers generously provide through Medicaid.
Other people finance long-term care with private resources and have no
need for taxpayer dependency. Many others have savings and investments
that could be used for long-term care but instead have taxpayers pay for
their long-term care, while protecting money and assets to pass onto their
heirs. Inadequate eligibility requirements and low pursual of
estate-recovery measures make this easier to do.
Medicaid is the primary payer of long-term care (LTC)
services in the nation and Washington state, and LTC funding makes up 20%
of Washington state Medicaid spending. Keeping up with the financial
demands to come from an increased number of people relying on taxpayers
for long-term care requires changes to eligibility requirements and estate
recovery measures attached to the safety net.
Key Takeaways
- Washington state is aging, and an
increasing number of people are applying for Medicaid long-term care (LTC)
earlier. This will lead to longer durations of use and escalating costs.
- LTC costs consumed 20% of $29.2
billion in Medicaid spending in Washington state in fiscal year 2022.
- Medicaid enrollees who used
long-term services and supports comprised 6% of total enrollment but 37%
of federal and state spending.
- The WA Cares Fund is unlikely to
substantially help reduce Medicaid LTC demand. Given a lifetime benefit
of $36,500, high LTC costs and irresponsible state messaging, program
recipients will often exhaust the benefit and then seek Medicaid.
- Medicaid is the primary payer for
LTC nationally, financing more than half (61%) of the total
spending. This reliance on taxpayers is concerning as the population
ages and program eligibility remains broadly accessible.
- Eligibility rules let people
rearrange assets to appear poor and qualify for taxpayer-funded
long-term care, even when they have nearly $1.1 million in home equity.
- Estate recovery helps repay
taxpayers after a recipient’s death, supporting program integrity and
sustainability, yet Washington recovered only 0.34% of $5 billion in
fiscal year 2025.
- To deter gaming and preserve aid
for those truly in need, lawmakers should push Congress to extend the
five-year asset look-back period to 20 years.
- Medicaid needs to be a safety net —
not an inheritance-preservation vehicle — protecting resources for
vulnerable Washingtonians.
READ THE FULL STUDY HERE
#############################
Updated
Monday, October 20, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC E-ALERT #25-038: LTC NEWS AND COMMENT
LTC Comment: Do you spend hours searching
the internet for useful articles, key data, and relevant reports to keep
you on the forefront of professional knowledge? Do you lose business
because you’re blindsided by clients or competitors who learn critical
information before you do? Here’s an antidote:
LTC Clippings: The Center for Long-Term
Care Reform notifies subscribers to our LTC Clippings service daily of
information you need to know. Each message contains only the critical
facts about new publications: a title, representative quote, a link to
the original, and our analysis in a sentence or two. To inquire or
subscribe, contact Damon at 206-283-7036 or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC E-Alerts: Once a week, we compile our
daily LTC Clippings into a summary, email it to Center for Long-Term Care
Reform members, and archive it in The Zone, our password-protected
members-only website. Center members also receive our weekly LTC Bullet
op-ed. To join the Center and receive all these benefits and more,
contact Damon at 206-283-7036 or
damon@centerltc.com.
We no longer post our LTC E-Alerts on the
Center’s public access website, but here’s what today’s LTC E-Alert
contained: links, quotes and comments on the following articles, reports,
or data:
-
Say what? Insensitive comments fuel family
caregiver’s humorous web video series
-
Seniorly to be acquired by CareScout in $20 million
transaction
-
How the Government Shutdown Could Affect Older
Adults
-
Impact Of The Carer's Gap
-
US adults are generally unprepared for aging, new
‘longevity preparedness index’ finds
-
US health agency releases 2026 quality ratings for
Medicare plans
-
Here’s what’s really stopping Medicare Advantage
from covering all of America’s seniors
-
Economic volatility driving people to delay
retirement or go back to work
-
Nationwide launches CareMatters Annuity to Address
Growing Long-Term Care Concerns
-
CBD Calms the Inflamed Alzheimer’s Brain
-
RN turnover in skilled nursing reaches 100 percent
over a decade
-
Out of pocket payments for home-based long-term
care in Europe drive older people into poverty
#############################
"LTC E-Alerts" are
a
feature offered by the Center for Long-Term Care Reform, Inc. to members
at the $150 per year level or higher. We'll track and report to you news
and analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Monday, October 13, 2025,
10:03 AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-037:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
2026 Tax Deductible Limits For Long-Term
Care Insurance Increase 3 Percent
-
Layin' it on the Line: The long-term care
crisis - why the government may force you to buy coverage
-
Largest Study of Alzheimer’s in African
Americans Reveals Disease Targets
-
Vote ‘Yes’ to strengthen WA Cares Fund for
elder, long-term care | Editorial
-
A small think tank's crusade against
Obamacare is making some Republicans nervous
-
Most Americans expect to need long-term
care in the future, and they don’t want that care in assisted living
-
Retirement goals slipping away as more
Americans live paycheck to paycheck
-
Senior living and care market sees
resurgence, increased demand
-
A small think tank's crusade against
Obamacare is making some Republicans nervous
-
Vote ‘Yes’ to strengthen WA Cares Fund for
elder, long-term care | Editorial
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Friday, October 10, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC BULLET: MEDICAID MONEY MANIPULATION HARMS
LONG-TERM CARE
LTC Comment: State Medicaid programs,
Medicaid planners, and the federal government manipulate money
mischievously in different, but complementary ways to the detriment of the
program’s mission. We explain after the ***news.***
|
*** TODAY'S LTC BULLET is sponsored by Claude
Thau (BackNine Insurance). BackNine gives you a free
personalized website at no cost. Your clients (& family & friends)
can, with as little or as much of your involvement as you or they
want, buy life insurance and LTCi, and can speed issue by scheduling a
paramed and uploading medical records immediately. We quote
stand-alone LTCi, linked-benefit and life with a LTC rider
side-by-side. Claude is the lead author of Milliman’s annual Broker
World LTCi Survey & a past Chair of the Center for Long-Term Care
Financing. Contact him at 913-707-8863 or
claude@back9ins.com to learn about more
great BackNine features and services. *** |
***
REGISTRATION IS NOW OPEN for the 2026 Intercompany Long Term Care
Insurance Conference! Organizers report: “Our in-person conference March
8-11, 2026 at the
Rosen Shingle Creek in Orlando, FL is now accepting attendee
registrations! As always, our
agenda will include numerous educational sessions over two days across
seven tracks with ample time for networking and reconnecting with
colleagues. We still have room for
exhibitors and
sponsors! Please contact us at
info@iltciconf.org if you are interested in either opportunity to
showcase your products and services to our attendees. Everyone who's
anyone in Long Term Care Planning will be there. What about your company?”
***
LTC BULLET:
MEDICAID MONEY MANIPULATION HARMS LONG-TERM CARE
LTC Comment:
State Medicaid programs employ provider taxes, intergovernmental transfers
and other creative financing methods to transfer costs from their general
funds onto federal taxpayers. Medicaid planners manipulate Medicaid
financial eligibility rules to qualify their affluent clients artificially
for Medicaid’s best care to the exclusion of the poor. The state and
federal governments convert high private LTC revenue into less-than-cost
Medicaid reimbursements to the detriment of care access and quality for
the poor and vulnerable the program is supposed to serve. This
concatenation of poor public policies got under my skin. I wrote the
following essay to tease out their meaning and consequences.
“Medicaid Money
Manipulation Harms Long-Term Care”
by
Stephen A. Moses
The Medicaid
program is big and growing rapidly. States administer Medicaid; the
federal government oversees their programs; both share the cost. States
contribute a payment that their federal partner matches by a formula
varying from 50% (one-to-one) to 83% of the total cost. States manipulate
this system with various creative financing techniques. For example,
nearly all states (49) tax health care providers to generate extra
revenues they use to boost their federal financial match without drawing
on their general funds. The Paragon Health Institute calls this and other
similar methods to maximize federal expenditures at minimal state cost,
often diverting them to unauthorized purposes, “legalized money
laundering.”
The largest
laundered sums involve hospitals and managed care insurers, but states
also tax nursing homes and other long-term care (LTC) providers for the
same purpose. Less understood is a related form of money laundering.
Non-poor people routinely qualify for Medicaid LTC benefits. Medicaid
converts their potentially higher private-pay revenue into below-cost
payments to LTC providers with serious negative consequences for care
access and quality. This paper discusses each of these Medicaid money
manipulation methods and their results.
Long-Term
Care
LTC consumes a
disproportionate share of Medicaid. Only six percent of Medicaid
recipients use LTC, but they consume 37 percent of program expenditures.
Although home and community-based services (HCBS) now consume nearly
two-thirds (63.2 percent) of Medicaid LTC spending,
nursing homes remain a critical care venue, serving 24 percent of all
Medicaid LTC recipients.
Forty-nine
states tax nursing homes, maximizing their federal match and laundering
funds for expanded uses. Despite measures implemented to control this
practice, the sums involved are very large. The Paragon Health Institute
cites a particularly egregious example in Indiana.
But more than
just money is involved. New research indicates that the LTC provider tax
gimmick may have far-reaching detrimental impacts on the access to and
quality of care Medicaid recipients receive.
Creative LTC
Financing
A recent NBER
working paper, titled “Creative Financing and Public Moral Hazard:
Evidence from
Medicaid and the Nursing Home Industry,”
argues that creative financing schemes like provider taxes have several
negative secondary effects. The authors conclude that such schemes distort
state incentives “discouraging increases in effective reimbursement rates
retained by the providers, while encouraging expanded access to inpatient
care.” (p. 35) They therefore exacerbate “the persistently low effective
Medicaid reimbursement rates that contribute to the systematic quality
shortfalls in the nursing home industry.” (p. 36) Simultaneously, “the
schemes incentivize higher inpatient care volume,” (p. 36) which the
authors call “public moral hazard,” despite “widespread preferences among
older adults to age at home.” (p. 36) Worst of all, they “show that
creative financing leads to disproportionate increases in Medicaid funded
care in the lowest-quality nursing facilities, with potentially harmful
consequences for patients.” (p. 1) According to the authors, dementia
patients in low quality facilities are disproportionately impacted.
Wholesale
Medicaid Money Laundering
In summary, the
new NBER paper finds that taxing LTC providers to increase federal
matching funds incentivizes states to (1) expand nursing home care volume
in preference to the HCBS that patients prefer, (2) channel funds
disproportionately to lower quality nursing homes serving many dementia
patients, and (3) capture some of the added federal funds for purposes
other than LTC, thus reducing effective nursing home reimbursement rates
and exacerbating related access and quality problems. Provider taxes
operate as a kind of wholesale money laundering scheme to capture extra
federal funds, redirect them from their intended use to other purposes,
increase LTC use and expenditures, and transfer the cost from state to
federal tax payers.
Retail Money
Laundering
Provider taxes
may also encourage money laundering at a retail level. The NBER paper
observes that “States can influence care volume through capacity
regulations, Medicaid eligibility, benefit design, and Home- and
Community-Based Services (HCBS) waivers.”
(Emphasis added) How might states increase caseloads by manipulating
Medicaid financial eligibility rules for the purpose of gaining more
federal matching funds? States have wide discretion to set and enforce
rules governing eligibility for Medicaid LTC benefits. They decide, for
example, how much countable wealth to allow recipients to retain; which
kinds of assets are exempt and in what amounts; to what extent they
enforce restrictions on asset transfers, irrevocable trusts and compliant
annuities to qualify; the level of effort they extend to track and collect
estate recoveries; and many others. Could it be that the incentive to
increase Medicaid LTC caseloads created by the provider tax scheme
contributes to the indifference many states show toward setting and
enforcing strict financial eligibility controls?
California is
an outlier in this regard, having totally eliminated its countable asset
limit for a time, and leaving in effect its most generous limit in the
country.
But few states successfully restrain access to Medicaid LTC benefits by
people with assets they could use to pay privately for their care.
Although Americans hold $97 trillion in retirement savings ($40T),
home equity ($35T),
and life insurance ($22T),
very little of that wealth goes to pay for their LTC. Only 6.5 percent of
the $629 billion they spent on LTC in 2023 came from private savings.
Medicaid (44 percent), Medicare (16 percent), private insurance (10
percent), other third party payers (17 percent), and private income of
people already on Medicaid (6.5 percent) paid the rest. In essence, most
potential private LTC spending is converted, or effectively laundered, to
become public spending mainly through Medicaid and Medicare with serious
consequences for LTC services and financing.
Combined LTC
Money Laundering
States and the
federal government are complicit in laundering private funds to convert
them to public expenditures. Federal financial eligibility rules
discourage states from controlling access to Medicaid LTC benefits by the
middle class and affluent. Provider tax incentives predispose states not
to exercise such control. The federal government requires that state
Medicaid programs treat many large assets as exempt. Examples include home
equity, side businesses, retirement savings, home furnishings, personal
belongings and many more. But federal law and regulations place no
restriction on spending down countable assets to purchase exempt resources
effectively obviating the need for prosperous people to spend their own
funds on care. “Medicaid’s $100+ Billion Leak” explains how this loophole
works and its consequences.
This policy of
diverting private LTC spending into public expenditures has devastating
consequences for LTC access and quality. It diverts hundreds of billions
of dollars of LTC spending from coming to care providers at market rates.
Channeling that spending through Medicaid causes providers to receive the
funds at egregiously low reimbursement rates, less on average than the
cost of providing the care.
This inadequate revenue is a primary cause of caregiver shortages that
lead to widespread access and quality problems. Faced with unsustainably
low reimbursements for nearly two-thirds of their residents,
nursing homes charge a dwindling supply of private payers rates above the
market-based rates that would apply in Medicaid’s absence. This
incentivizes the remaining private payers to find ways to qualify for
Medicaid without spending down assets.
Medicaid’s
Mission Redefined by LTC Money Laundering
Medicaid is
supposed to be a safety net for people in need of LTC but unable to pay
for it. But Medicaid LTC money laundering at the wholesale, retail and
combined levels has made a mockery of that mission. States fleece the
federal government with provider tax schemes. Federal eligibility laws and
regulations enable the middle class and affluent to access LTC benefits
without spending down assets. Savvy financial advisers direct prosperous
clients to take full advantage of the loose financial eligibility rules.
At the same time, Medicaid’s income and asset spend down rules quickly
crush the poor, aged and vulnerable with high private pay outlays they
have no way to avoid.
In recent
years, the Affordable Care Act (ACA) further undermined Medicaid’s LTC
safety net role by extending benefits to able-bodied, working-age
recipients up to 138 percent of the poverty level. The 90 percent federal
match for these “expansion” enrollees incentivized states to shift
eligibility and spending to that group leaving the traditional poor and
vulnerable caseload shortchanged.
In 2003, the aged and disabled were 25 percent of enrollees and they
consumed 69 percent of total Medicaid expenditures.
By 2022, this needier group had declined to 20 percent, receiving only 51
percent of total spending.
The poorest of the poor, “dual eligibles” who qualify for both Medicaid
and Medicare, were 14 percent of Medicaid enrollees in 2005 and accounted
for 42 percent of total program expenditures.
By 2023 they remained 14 percent of enrollees but they garnered only 32
percent of spending.
These changes reflect the ACA’s redirecting Medicaid toward able-bodied,
working-age recipients to the detriment of the more vulnerable aged and
disabled.
Conclusion
Creative
financing schemes used (1) by state Medicaid programs, such as provider
taxes (wholesale); (2) by individual affluent recipients and their
financial advisers, such as gaming Medicaid financial eligibility rules
(retail), and (3) by both, such as diverting LTC funding from the private
market sector to Medicaid funding (combined), increase federal Medicaid
LTC expenditures excessively, divert federal funds to unintended and
unauthorized purposes, and impair the access to and quality of care
available to the public.
Congress should
recapture control of Medicaid LTC financing by (1) ending the provider tax
gimmick, (2) closing the financial eligibility loopholes that convert
Medicaid LTC from a safety net for the needy to a hammock for the middle
class, and (3) using the savings therefrom to ensure Medicaid pays LTC
providers market-based rates for a much smaller caseload of genuinely
needy recipients. Further savings will accrue as these changes work their
way through the market incentivizing more aging Americans to take the risk
and cost of LTC seriously, plan ahead, save, invest or insure for LTC, and
stay off Medicaid.
#############################
Updated Monday, October 6, 2025,
10:03 AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-036:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Why fewer seniors are expected to enroll in
Medicare Advantage next year - and opt for original Medicare instead
-
Malpractice claims involving nurses on the rise in
home healthcare, report finds
-
Occupancy increases for 17th quarter in a row as
boomers fill up senior living communities ‘faster than they can be
built’: NIC
-
What the Trump Administration Can Do in the
Short-Term to Address the Long-Term Care Crisis
-
CareScout launches long-term care insurance option
-
CareScout Launches Care Assurance, First Insurance
Solution for Company
-
Protecting Your Inherited Home From Long-Term Care
Costs: The Basics
-
Veterans with burdened caregivers more likely to
enter nursing homes, study finds
-
KFF study: A look at growing enrollment in Medicare
Advantage special needs plans
-
Pay gap getting bigger, ADP says
-
China:New guidelines for long-term care insurance
services
-
Who'll Take Care of Grandma? How Trump's
Immigration Policies Threaten Elder Care
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Monday, September 29, 2025,
10:03 AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-035:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Americans risk retirement security to
support loved ones, study finds
-
I Asked ChatGPT How a 55-Year-Old Can
Prepare for Retirement, Here's What It Said
-
Study Sheds Light on Drinking and Dementia
Risk
-
Home care job openings expected to
skyrocket amid wage pressures, job instability
-
Study uncovers communication gaps between
long-term care insurers, family caregivers
-
States Are Cutting Medicaid Provider
Payments Long Before Trump Cuts Hit
-
Alliance urges policymakers for ‘bold’
action to correct HCBS rate insufficiency
-
Physical frailty may cause dementia, study
suggests
-
Average Spending by Age for Those 55 and
Up: Are You Thrifty?
-
U.S. Retirement Assets Hit Record $45.8
Trillion In Second Quarter 2025
-
Nursing homes fail to report 43% of major
falls: Behind OIG’s findings
-
Layin’ It on the Line: The hidden IRS rule
that could save your retirement from long-term care costs
-
66 percent of millennials, Gen Z expect to
inherit $335K from parents in ‘Great Wealth Transfer’
-
New Study Finds Families with Long-Term
Care Insurance Face Less Financial Strain
-
Longer Pre-SNF Hospital Stays More Likely
For Medicare Advantage Beneficiaries
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Friday, September 26, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC BULLET: LTC POLICY GOES AROUND AND COMES AROUND
LTC Comment: The last year long-term care financing
policy and Medicaid LTC reform were major political issues was 2005. What
goes around comes around, after the ***news.***
*** ATTENTION:
ILTCI ’26. The next Inter-Company Long-Term Care Insurance Conference will
be held March 8-11, 2026 in Orlando, Florida. Exhibitor and sponsor
applications are available now and attendee registration opens online with
early bird pricing October 1st. As usual, Steve and Damon from
the Center for Long-Term Care Reform look forward to attending this
essential LTC industry event. Join us, and in the meantime, go to
ILTCICONF.ORG
for further
information. ***
*** “What goes around comes around,” and thanks to
our members, the Center for Long-Term Care Reform stays around. Please
join us in our mission to ensure quality long-term care for all Americans.
We do this by promoting public policy that targets scarce public resources
to the neediest, while encouraging people who are young, healthy and
affluent enough, to take responsibility for themselves. To find out how
you can "do well by doing good," consider supporting our work by joining
us at the Premium Membership level. Center for Long-Term Care Reform
premium members receive our full suite of individual membership benefits
including:
· All LTC
Bullets and E-Alerts
· Access
to our Members-Only Zone website and Almanac of Long-Term Care
·
Subscription to our Clipping Service
·
Email/phone access to Steve Moses for 24-hour turnaround queries
Our Premium Membership is designed to give you a competitive advantage
in your long-term care profession. Your increased knowledge of the
critical issues and challenges we face in the field of long-term care
service delivery and financing equals improved professional success for
you and better LTC services for your clients and for those who have no
choice but to rely on scarce public resources.
Stay on the forefront of professional knowledge and
help us fight for rational long-term care policy reform by contacting
Damon at 206-283-7036 /
damon@centerltc.com to start your Premium Membership immediately or go
directly to our secure online subscription page and
sign up for as little as $21 per month. ***
LTC BULLET: LTC POLICY GOES AROUND AND COMES AROUND
LTC Comment: Join me today for a ride in the
Cato Institute’s way-back machine. The libertarian think tank has
recovered a long-lost video of a 2005 debate. The battle of wits pitted
free-market advocate
Steve Moses against Medicaid estate planner
Vincent Russo. Cato’s Director of Health Policy Studies,
Michael F. Cannon, introduced the program.
Marilyn Werber Serafini, then an award-winning journalist with the
National Journal, moderated. Watch the debate
here. (Click the picture on the right when the website comes up.)
Watch the video and you’ll note I got some things
wrong. I predicted that federal and state budgets were approaching a
breaking point. I said Medicaid and Medicare were at risk. In the future,
I thought people would not be able to ignore the risk and cost of LTC
until they need care and then turn the liability over to Medicaid. Home
equity would become the main funder of LTC for the majority of elderly who
were home owners. Private LTC spending and insurance would flourish as the
only path to quality LTC, especially in home and community-based settings.
Boy was I wrong back then. What happened instead was
that Medicaid LTC spending continued to grow. Medicaid financial
eligibility remained easy. LTC insurance sales slumped dramatically.
Medicaid’s giant home equity exemption continued to crowd out private LTC
financing through home equity conversion. All the things I warned were
ruining LTC access and quality back then only became worse over the next
two decades. Hope for change languished.
How can we explain those last twenty years? 2005 was
a heady year for LTC financing policy. The economy was good, but
politicians fought over Medicaid spending, especially LTC expenditures.
The big LTC issues were resolved when the Deficit Reduction Act became law
in March of 2006. The DRA established the first ever cap on Medicaid’s
home equity exemption and made asset transfer restrictions longer and
stronger. It seemed like my predictions and recommendations were coming
true.
Unfortunately, 2005 was the last year that Medicaid
and LTC financing costs dominated political discussion. Since then, there
have been studies and proposals, mostly advocating big new state and
federal LTC entitlements, but spending has surged instead in the existing
dysfunctional system with no relief. For the past twenty years, worries
about budget deficits and escalating debt subsided, enabling the status
quo to continue and worsen. Consequently, the national debt exploded from
$8.1 trillion in 2005 to $37.5 trillion today.
But politicians’ casual attitude about deficits and
debt is changing now. Budget constraints that dominated in 2005 are
finally returning in 2025. Inflation has exceeded the Fed’s 2% goal for
nearly five years and will continue high until 2028 at least. In FY 2024,
the federal government spent $6.75 trillion, but collected only
$4.92 trillion in revenue, causing a $1.83 trillion deficit. Analysts
worry the U.S. will be unable to service the national debt as interest
payments alone already exceed spending for national defense.
So, I stand by my predictions and recommendations
from that long-ago debate. The economic reckoning I predicted then is
finally upon us. We may flounder on a little longer, but by the mid-2030s,
the end will come for the LTC financing system that has prevailed since
Medicaid’s founding in 1965. 2031 marks the year boomers start turning 85
and their health and LTC needs skyrocket. Social Security’s trust fund is
exhausted in 2034; Medicare’s in 2033. Both those entitlements prop up
Medicaid LTC, but won’t help much going forward.
If you want to know what all this means, watch that
2005 debate again. I stand by what I said then. What’s different is
that the denouement I predicted in 2005 is closer than ever now. What goes
around, comes around, and, boy, is it coming at us hard and fast today.
#############################
Updated
Monday, September 15, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC E-ALERT #25-034:
LTC NEWS AND COMMENT
LTC Comment: Do you spend hours searching
the internet for useful articles, key data, and relevant reports to keep
you on the forefront of professional knowledge? Do you lose business
because you’re blindsided by clients or competitors who learn critical
information before you do? Here’s an antidote:
LTC Clippings: The Center for Long-Term
Care Reform notifies subscribers to our LTC Clippings service daily of
information you need to know. Each message contains only the critical
facts about new publications: a title, representative quote, a link to
the original, and our analysis in a sentence or two. To inquire or
subscribe, contact Damon at 206-283-7036 or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC E-Alerts: Once a week, we compile our
daily LTC Clippings into a summary, email it to Center for Long-Term Care
Reform members, and archive it in The Zone, our password-protected
members-only website. Center members also receive our weekly LTC Bullet
op-ed. To join the Center and receive all these benefits and more,
contact Damon at 206-283-7036 or
damon@centerltc.com.
We no longer post our LTC E-Alerts on the
Center’s public access website, but here’s what today’s LTC E-Alert
contained: links, quotes and comments on the following articles, reports,
or data:
-
Federal long-term care advisory commission proposed
-
CCRC operations have stabilized, but SNF-heavy ones
face issues, Fitch says
-
Senior living helps older adults live well longer,
NORC/NIC study finds
-
From early detection to advanced care: How IoT is
reshaping Alzheimer’s management
-
Who Pays for Long-Term Services and Supports?
-
Expanding the scope of extended care to ease the
growing healthcare burden
-
Risky Prescribing and the Epidemic of Deaths From
Falls
#############################
"LTC E-Alerts" are
a
feature offered by the Center for Long-Term Care Reform, Inc. to members
at the $150 per year level or higher. We'll track and report to you news
and analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Tuesday, September 9, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC E-ALERT #25-033:
LTC NEWS AND COMMENT
LTC Comment: Do you spend hours searching
the internet for useful articles, key data, and relevant reports to keep
you on the forefront of professional knowledge? Do you lose business
because you’re blindsided by clients or competitors who learn critical
information before you do? Here’s an antidote:
LTC Clippings: The Center for Long-Term
Care Reform notifies subscribers to our LTC Clippings service daily of
information you need to know. Each message contains only the critical
facts about new publications: a title, representative quote, a link to
the original, and our analysis in a sentence or two. To inquire or
subscribe, contact Damon at 206-283-7036 or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC E-Alerts: Once a week, we compile our
daily LTC Clippings into a summary, email it to Center for Long-Term Care
Reform members, and archive it in The Zone, our password-protected
members-only website. Center members also receive our weekly LTC Bullet
op-ed. To join the Center and receive all these benefits and more,
contact Damon at 206-283-7036 or
damon@centerltc.com.
We no longer post our LTC E-Alerts on the
Center’s public access website, but here’s what today’s LTC E-Alert
contained: links, quotes and comments on the following articles, reports,
or data:
-
Why Bruce Willis's Family Moved Him into a Separate
Home
-
Affluent Investors Are Embracing
"Multi-Retirements"
-
How will Medicaid changes affect long-term care?
-
‘Sandwich Generation’ Neglecting Retirement Savings
-
Nebraska Town Says CON Laws Are Blocking Nursing
Home Care
-
BREAKING: CMS intends to repeal nursing home
staffing rule
-
Social Security and Medicare cuts are coming
because the bond market will eventually bring Congress to its knees,
economist says
-
Is Life Insurance The Answer To The Growing
Long-Term Care Need In The U.S?
-
Study finds accumulated wealth dramatically reduces
dementia odds in seniors over 80
#############################
"LTC E-Alerts" are
a
feature offered by the Center for Long-Term Care Reform, Inc. to members
at the $150 per year level or higher. We'll track and report to you news
and analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Friday, September 5, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC BULLET: HOW TO FUND WISH
LTC Comment: Analysts and advocates have rallied
around WISH, but the proposed LTC insurance plan is starved for funding.
Where could the needed money come from?
LTC BULLET: HOW TO FUND WISH
LTC Comment: New York Congressman
Tom Suozzi has introduced the Well-Being Insurance for Seniors to be
at Home (WISH) Act. It is a creative new approach to funding long-term
care that has captured the imagination and gained the support of many LTC
analysts, advocates, providers, and insurers. I’ve criticized the plan
here and
here. But that is not my purpose today. Rather, I’d like to say “if
this is what you want to do, here’s how to pay for it.”
What is WISH?
In briefest summary, WISH proposes a new catastrophic
or back-end LTC insurance program that would pay qualified recipients a
cash benefit equal to the median cost of six hours per day of personal
care. To qualify, participants would have to meet their own LTC costs
during a waiting period of one to five years depending on their income.
Higher income people would pay their own way longer than lower income
people before qualifying. WISH also plans a major public education
campaign; expects private insurers to wrap new, less expensive policies
around the WISH chassis; and hopes that Medicaid savings will accrue.
The catch is how to pay for WISH. Earlier proposals
included a mandatory payroll deduction of three percent from workers and
three percent from employers. In the current economic and political
climate, that plan proved impractical. With the national debt exceeding
$37 trillion, interest rates and inflation on the increase, and
America’s creditors balking at buying our bonds, the country’s ability to
service the debt it already has is at risk. As federal expenditures
already far exceed revenue, any additional spending must be borrowed or
printed, further worsening the financial crisis. So, if payroll taxes are
out, where could the money come from to support WISH?
Finding New LTC Money
Medicaid allows LTC recipients to retain substantial
wealth in exempt form. Exempt assets include up to a million dollars in
home equity; the cost of home upgrades; one business including the capital
and cash flow; an automobile; personal service contracts; unlimited home
furnishings and personal belongings; compliant annuities and promissory
notes; and even IRAs if they are in payout status, as most are for the
elderly due to required minimum distributions (RMDs). No one knows how
much wealth Medicaid LTC recipients own in this exempt form. But it is
likely very substantial because of a quirk in Medicaid financial
eligibility rules that encourages conversion of countable assets into
exempt status.
Artificial Asset Spend Down
Medicaid treats asset spend down differently than
income spend down. To reach the maximum monthly income limit of $967
dollars, applicants must demonstrate that they have purchased qualified
medical or LTC goods or services with their own funds. The same is not
true for asset spend down. To reach the $2,000 asset limit that applies in
most states, applicants may spend their excess funds on anything they
choose as long as they receive fair market value in return. They do not
have to purchase qualified medical or LTC goods or services. In fact, they
can buy assets that Medicaid considers exempt. This gives Medicaid LTC
applicants a strong incentive to “spend down” by converting their
countable assets into exempt resources with a simple purchase. There is no
practical limit on how much wealth Medicaid LTC recipients can shelter
from actual spend down in this way.
Medicaid’s well acknowledged proper role is to be a
LTC safety net for the poor and vulnerable. It is supposed to protect the
middle class and affluent only after they have consumed their excess
resources by purchasing their own care. The presumption that genuine spend
down of assets for LTC will occur is a key element of the WISH program. It
follows that we need to know how much private wealth Medicaid protects in
exempt form and how common the practice of spending down countable wealth
by purchasing exempt resources is. What if the sums are so large and the
practice so common that Medicaid has effectively obviated the need for
middle class and affluent people to spend substantial personal funds for
their long-term care? This could explain why so few people plan early,
save, invest or insure for LTC. If the worst happens, Medicaid pays and
protects significant wealth.
Clues from GAO
We have more questions than answers, but here are
some clues. GAO conducted a
study in 2014 that attempted to estimate the amount of exempt assets
Medicaid LTC recipients own. GAO’s findings were not “generalizable” to
the whole country due to limits in their methodology. But in a paper for
the
Paragon Health Institute titled “Medicaid’s
$100+ Billion Leak,” I asked “what if GAO’s findings were projectable?
How much money lies fallow, unused to purchase private LTC, because
Medicaid exempts that wealth and pays the bills instead?” The sums were
impressive. For example:
-
“Half or more of Medicaid’s $217 billion annual LTC
budget [$278 billion as of 2023] goes to beneficiaries who could
otherwise afford to pay privately.”
-
“Medicaid covered 5.6 million LTC recipients in
2020. If 12.6 percent of them had over $100,000 in noncountable
resources, as GAO found, then at least $70.4 billion went unused for
private LTC financing at Medicaid’s expense. That’s a lot of wealth for
a poverty program to protect, fully 32.5 percent of the total $217
billion Medicaid spent on LTC.”
-
“If [as GAO found] 75 percent of LTC recipients
owned a median amount of $12,530 in noncountable assets each, then at
least $52.6 billion found its way into sheltered wealth, largely as
prepaid burial expenses, which are sometimes permitted for the entire
family, including adult children. That is a giant subsidy for the
funeral industry at the expense of LTC financing for the poor, fully
24.2 percent of total Medicaid LTC expenditures.”
-
“If [according to GAO] 31 percent of 5.6 million
Medicaid recipients owned homes with a median value of $68,350, then
$118.7 billion of real estate value was diverted from private LTC
financing. (The $68,350 is from the GAO report and would be much higher
if the analysis was done today and not a decade ago.) Given that
Medicaid exempts nearly all home equity, it is clear that Medicaid
replaces practically all personal LTC liability from home equity. The
loss is 54.7 percent of what the program spends on LTC.”
That is a lot of money (54.7 percent of 2023 Medicaid
LTC expenditures [$278 billion] would be $152 billion) that Medicaid
protects from the cost of paying privately for LTC. But what if the actual
amount is much higher? GAO analyzed the total of exempt assets in only two
counties in each of three states, Florida, New York and South Carolina.
They researched and analyzed only a small sample of 350 cases. GAO based
its findings on case record reviews and interviews with eligibility
workers, but it did not verify the completeness and accuracy of the case
records by reviewing bank accounts or public records, such as property
ownership or transfers. Given these shortcomings, and others GAO
acknowledges in this and other reports, it is safe to say that this study
found only a fraction of the exempt assets that the Medicaid recipients
possessed.
Follow the Money
To identify funds that could be tapped to fund WISH,
Congressman Suozzi should ask GAO and CBO to conduct comprehensive studies
of (1) the kind and amount of exempt assets held by Medicaid recipients in
the United States and (2) the extent of the practice of qualifying for
Medicaid LTC benefits by purchasing exempt assets to spend down countable
wealth.
These studies should …
-
Review sample sizes sufficient to generalize
results to the whole U.S. population.
-
Include critical review of case records, followed
by interviews with Medicaid eligibility workers, supervisors, recipients
and family members.
-
Review public records such as county assessors
(real property ownership) and recorders (property transfer).
-
Conduct matches with IRS, Social Security, and
other data bases to find unreported assets.
Verify the incidence and equity value of home ownership by Medicaid LTC
recipients.
Home equity incidence and amount is especially
important to determine because it is currently unknown, likely very high
and could easily be used to reduce Medicaid expenditures, saving money
WISH could employ, if Congress required home equity conversion as a
condition of eligibility.
Make Asset Spend Down Real
Once we know how much exempt wealth Medicaid protects
from actual LTC spend down, Congress should consider making two changes in
Medicaid financial eligibility policy.
-
Change the asset spend down rules to comport with
the income spend down requirements. In other words, require that asset
spend down be for qualified medical or LTC expenses as is already
mandatory for income spend down.
-
Disallow the practice of purchasing exempt assets
to reduce countable wealth artificially.
These measures would likely not entirely replace the
revenue WISH could have generated from a payroll tax, probably around $530
billion per year, but they would vastly relieve the burden on Medicaid of
funding LTC and substantially increase the incentive for the middle class
and affluent to plan for LTC, purchase private insurance, and stay off
Medicaid.
More to Come
Does it seem far-fetched that more than half of what
Medicaid spends on LTC, over $150 billion, could be protecting wealth that
people might otherwise have used to purchase quality care in the private
market? What if I told you that amount is dwarfed by the total wealth that
could go to fund private LTC, but doesn’t, because of various third
parties? To get the evidence and logic to support this claim, stay tuned
for a forthcoming LTC Bullet, provisionally titled “Better LTC for
Billion$ Less.” Coming this month.
Subscribe
Did someone forward today’s LTC Bullet to you?
Don’t miss any future LTC Clippings, LTC Bullets, or LTC
E-Alerts. Become a premium member of the Center for Long-Term Care
Reform
here. Thanks for your support.
#############################
Updated Monday, September 1, 2025,
10:03 AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-032:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
ALTCS Release on Support for Long-Term Care Bill
-
Sense of purpose protects against dementia, large
study finds
-
WISH Act could ‘substantially’ improve retirement
outcomes for those with catastrophic LTSS needs, analysis finds
-
Could ‘Golden Passport’ tempt older adults to swap
senior living for cruise ship living?
-
Failing to save enough for retirement is top
financial regret, survey finds
-
Public awareness campaigns needed to increase
long-term care insured rate, report says
-
My Mom Needs Nursing Home Care —Can She Cash Out
Her Annuity To Pay Off Her Mortgage And Still Qualify For Medicaid In
New York?
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Monday, August 25, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC E-ALERT #25-031:
LTC NEWS AND COMMENT
LTC Comment: Do you spend hours searching
the internet for useful articles, key data, and relevant reports to keep
you on the forefront of professional knowledge? Do you lose business
because you’re blindsided by clients or competitors who learn critical
information before you do? Here’s an antidote:
LTC Clippings: The Center for Long-Term
Care Reform notifies subscribers to our LTC Clippings service daily of
information you need to know. Each message contains only the critical
facts about new publications: a title, representative quote, a link to
the original, and our analysis in a sentence or two. To inquire or
subscribe, contact Damon at 206-283-7036 or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC E-Alerts: Once a week, we compile our
daily LTC Clippings into a summary, email it to Center for Long-Term Care
Reform members, and archive it in The Zone, our password-protected
members-only website. Center members also receive our weekly LTC Bullet
op-ed. To join the Center and receive all these benefits and more,
contact Damon at 206-283-7036 or
damon@centerltc.com.
We no longer post our LTC E-Alerts on the
Center’s public access website, but here’s what today’s LTC E-Alert
contained: links, quotes and comments on the following articles, reports,
or data:
-
Despite expectations of longevity, many retirees
unprepared for potential LTC needs
-
Dual eligibles still rely heavily on family for
care despite LTSS program expansion
-
Biden-era rule curbing Medicare Advantage marketing
incentives overturned
-
Bill Gates Backs $1M AI prize to Tackle Alzheimer’s
-
A Federal Backstop for Long-Term Services and
Supports Could Change Retirement Outcomes
-
CMS Launches Nationwide Push to Remove Ineligible
Medicaid Enrollees, Uphold Citizenship Requirements
-
States created Medicaid add-ons to protect access.
Nursing homes started taking more Medicare patients instead
-
Nearly one quarter of Americans financially support
aging parents: report
-
Senior living returns outperform all other real
estate sectors in first half of 2025
-
Why Are So Many Seniors Being Evicted From Their
Long-Term Care Homes?
-
Estate Planning: The latest regarding Medi-Cal’s
asset test
#############################
"LTC E-Alerts" are
a
feature offered by the Center for Long-Term Care Reform, Inc. to members
at the $150 per year level or higher. We'll track and report to you news
and analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Friday, August 22, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC BULLET: IS MEDICAID FOR THE POOR AND VULNERABLE?
LTC Comment: Medicaid is nearly always described as a
program for the poor and vulnerable. Is that true? Was it ever? Today, we
explore some evidence that suggests it wasn’t and isn’t, after the
***news.***
*** TAKE ACTION: Compiling and reviewing the content
of today’s Bullet brought to my mind these famous quotes.
"The only thing necessary for the triumph of evil is
for good men to do nothing".
"Silence in the face of injustice is complicity with the oppressor."
"If you are neutral in situations of injustice, you have chosen the side
of the oppressor."
Standing by while Medicaid is converted from a safety
net for the poor and disabled into a hammock for the financially
comfortable is a case in point.
If you want to be part of the movement to return
Medicaid to those who need it most and to incentivize everyone else to
take personal responsibility, especially for LTC planning, then join the
Center for LTC Reform and help us fight the good fight.
You can join and contribute
here. Thanks for your time and consideration. ***
LTC BULLET: IS MEDICAID FOR THE POOR AND VULNERABLE?
LTC Comment: How many articles have you read
that explain how Medicaid benefits the affluent, often to the exclusion or
disadvantage of the needy? Not many, I’ll bet, unless you follow these
LTC Bullets. But there is plenty of evidence that, to whatever extent
Medicaid was aimed at the poor and vulnerable originally, the program is
undergoing a major change in the opposite direction. I’ll summarize some
of that evidence below and use it as a base for a future article on the
topic.
Of course, the go-to source for evidence that
Medicaid LTC benefits are easily and widely available to non-poor
Americans is the Center for Long-Term Care Reform’s
articles, speeches, reports and newsletters (LTC
Bullets). Here are quotes from and links to a few recent examples
“Medicaid should help the poor, but crushes them. The
affluent should pay for their own LTC, but don’t. Then they take the best
Medicaid offers. What’s wrong and what to do?” (“Medicaid
Oversight,” July 11, 2025
“Is Medicaid LTC set up to hurt the poor,
underprivileged, and marginalized while inordinately benefiting the
affluent and middle class?,” (“Understanding
Structural Long-Term Care Racism,” May 16, 2025)
“Private wealth sits on the sidelines as Medicaid
shifts from helping the poor and vulnerable to subsidizing the middle
class and affluent. Facts and analysis follow.” (“How
the Wealthy Stole Medicaid,” April 18, 2025)
But Medicaid is not only available to the middle
class and affluent in need of long-term care. It has also come to
prioritize young, able-bodied people over the aged, poor, disabled, and
most vulnerable. The
Paragon Health Institute has identified a number of ways that Medicaid
has transitioned from covering the poor and vulnerable to covering many
more.
“For more than a decade, the Affordable Care Act’s (ACA)
Medicaid expansion has shifted resources away from the most vulnerable
Americans – single moms, infants, and the disabled – in favor of
able-bodied adults without dependents.” (“Losing
Focus: How the ACA’s Medicaid Expansion Left Traditional Enrollees Behind,”
by Liam Sigaud, February 10, 2025)
“Since 2013, Medicaid rolls have swelled under the
Affordable Care Act. More
than 20 million able-bodied, working-age adults to Medicaid. These new
enrollees, who now account for about 25 percent of Medicaid enrollees
nationwide, have put additional strain on the health care system and diverted
resources away from vulnerable Medicaid enrollees.(“Myth:
The OBBB will harm the most vulnerable Medicaid enrollees,” by Liam
Sigaud, August 5, 2025)
“The Affordable
Care Act (ACA)
significantly expanded Medicaid over the past decade, worsening the
program’s structural problems. The ACA created
a new eligibility category for Medicaid—able-bodied, working-age
adults—with a much higher federal reimbursement percentage for these
enrollees. This has led to a host of problems, including: 1) a diversion
of resources away from traditional Medicaid enrollees, particularly
low-income children and people with disabilities, that has reduced their
access to health care services; 2) a near quadrupling of Medicaid’s
improper payments; and 3) a surge of spending that has significantly
contributed to large and growing federal deficits.” (Medicaid
Financing Reform: Stopping Discrimination Against the Most Vulnerable and
Reducing Bias Favoring Wealthy States,” by Brian Blase and Drew
Gonshorowski, July 2025)
“States receive $9 in federal funds for every $1 of
state spending on able-bodied, working-age adults compared to an average
of only $1.33 in federal funds for every $1 of state spending on children,
pregnant women, seniors, and people with disabilities. Thus, states
receive nearly seven times more federal funding for every $1 of spending
on expansion enrollees than traditional enrollees. This incentivizes
states to prioritize expansion enrollees over traditional, more vulnerable
populations and harms
their access to care.” (“Consequences
of Medicaid’s Discrimination Against the Most Vulnerable,” by Brian
Blase, June 29, 2025)
“The week’s Paragon Pic highlights the significant
expansion in Medicaid enrollment over the last three decades,
demonstrating that it is no longer solely a safety net for categories of
just low-income Americans. … Paragon has written extensively on how Medicaid
expansion has led to many problems, including a diversion
of resources away from traditional Medicaid enrollees, a near
quadrupling of Medicaid’s improper
payments, and a surge of spending that has significantly contributed
to ballooning federal
deficits. Paragon also has written about how easy it is for people to
qualify for Medicaid long-term
care services, as the easy ability to artificially impoverish parents,
aunts, and uncles has enabled heirs to protect their inheritances and pass
costs to their fellow Americans.” (“Paragon
Pic: Medicaid is No Longer for the Poor,” by Drew Gonshorowski)
“Though Medicaid was intended to provide health care
for the truly needy, the federal government provides an open-ended federal
reimbursement of real state expenditures but also artificial state
expenditures. As a result, states, insurers, and providers have used
Medicaid to siphon hundreds of billions of dollars from federal taxpayers
over the past decade and raise payments well above what can be considered
‘economical or efficient,’ as federal law requires.” (“Addressing
Medicaid Money Laundering,” by Brian Blase and Niklas Kleinworth,
March 2025)
“Unrestricted Medicaid
Expansion: California uses this influx of federal money to fund
large-scale Medicaid expansions. The most significant of these are
extending Medicaid coverage to illegal immigrants and eliminating the
asset test so wealthy people can qualify for taxpayer-financed long-term
care. Because the federal dollars are money laundered, the state
circumvents restrictions on federal Medicaid funding for illegal
immigrants.” (“California’s
Insurance-Tax Shuffle: How Federal Money Ends Up Paying for Medicaid for
Illegal Immigrants,” Paul Winfree and Brian Blase, March 12, 2025)
“Medicaid, a vital program for indigent and disabled
Americans who need long-term care, is facing a crisis of sustainability.
The program, initially designed to assist those with insufficient means,
is commonly exploited by loopholes in the system that allow basically
anyone to gain eligibility for LTC services through financial planning.
This trend not only stretches Medicaid’s resources thin but also raises
questions about the program’s long-term viability and its impact on state
and federal budgets.” (“Preserving
long-term Medicaid for the poor,” Gary Alexander, January 15, 2024)
“For decades, federal policymakers of both parties
tried to ensure that scarce Medicaid LTC resources went solely to the
needy. They failed, leaving Medicaid, including state and federal budgets,
financially overwhelmed and most people, regardless of their economic
condition, using public assistance if they incur catastrophic LTC costs.”
(“Long-Term
Care: The Solution,” Stephen Moses, October 2023)
Closing LTC Comment: From 1965 until 1980,
Medicaid allowed everyone to give away unlimited wealth without penalty to
qualify for LTC benefits. Costs exploded, so measures were taken to
discourage improper asset transfers and eventually to require recovery of
exempt assets from estates. But none of those measures succeeded. Middle
class and affluent people gained access to Medicaid after they confronted
high LTC costs. Heirs benefited by Medicaid’s protecting their
inheritances. Consumers responded by failing to plan for LTC. Private LTC
insurance languished as a result. During Covid, Medicaid didn’t even
enforce the existing lenient financial eligibility rules exacerbating all
these problems. Since the Affordable Care Act, Medicaid has prioritized
serving young, able-bodied people with huge subsidies for them to the
detriment of aged, poor and disabled recipients. This whole house of cards
is destined to collapse. When it does, America will be forced to adapt to
an absence of huge, market distorting government transfers. Far better to
move in the direction of market-based LTC by thoughtful policy than to
wait for the economy to take us there by default. How to do that?
For analysis and ideas on LTC reform, read the
Paragon Health Institute’s “Long-Term
Care: The Problem” and “Long-Term
Care: The Solution” and watch this “virtual
LTC event” featuring age wave visionary Ken Dychtwald and leading LTC
researchers. To find ample private funds for LTC, check out “Medicaid’s
$100+ Billion Leak.” For what not to do, see “Medi-Cal-amity:
California’s Reckless Expansion of Medicaid Long-Term Care to the Affluent.”
Find much more on long-term care
here.
#############################
Updated Monday, August 18, 2025,
10:03 AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-030:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Genworth plans major move in fraught
long-term care insurance market
-
Ken Dychtwald’s Future Vision of Health,
Aging and Longevity
-
Should You Disown Your Assets to Get
Medicaid Long-Term Care? What to Know
-
The Rise of Phantom Obamacare Enrollees:
Biden COVID Credits Drive Massive Increase in Individual Market
Enrollees With No Medical Claim
-
Men with dementia face 24 percent higher
death risk than women in major Medicare study
-
300 million program to expand access met
with restrained enthusiasm by long-term care experts
-
How retirees can manage rising healthcare
costs
-
‘Groundbreaking’ companionship exemption to
give home care agencies better flexibility, attorney says
-
Long-Term Services and Supports in
Supplemental Benefits in Medicare Advantage Plans
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Monday, August 11, 2025,
10:03 AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-029:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
The Silver Tsunami
-
MA-specialized home health agencies deliver
less care, worse health outcomes, major study finds
-
Long-term care on track for a third of
healthcare bankruptcy case volume this year
-
Foreign-Born Workers Made Up Half The
Increase In The Direct Care Workforce In Home And Community Settings,
2012–22
-
Study: Mental health problems plague nearly
half of nursing home staff
-
Surgical care through Medicare Advantage is
lower cost and does not compromise patient safety, new major study finds
-
Study: Medicare spends billions on
medically unnecessary procedures
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Friday, August 8, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC BULLET: LTC MUSINGS
LTC Comment: Three weeks of wandering around East
Africa with hardly a thought about long-term care left me reflecting on
four decades of struggling with that intractable public policy challenge.
Some thoughts after the ***news.***
*** LTC CLIPPINGS: Did you catch these
stories this week? Our LTC Clippings subscribers received them in
real time including Steve Moses’s always trenchant, often ironic,
sometimes humorous, usually concise “LTC Comments.” To subscribe or for a
free trial, contact Damon at 206-283-7036 or
damon@centerltc.com. Examples below:
8/2/2025, “Study:
Medicare spends billions on medically unnecessary procedures,” by
Donna Shryer, McKnights LTC News
Quote: “A new study reveals
that Medicare beneficiaries are receiving billions of dollars worth of
medical care that offer little to no clinical benefit and may lead to
harm. Researchers found that Medicare spent $4.4 billion annually between
2018 and 2020 on 47 different low-value medical services, with seniors
paying an additional $800 million out of their own pockets.”
LTC Comment: When government is the payer, the provider is the
customer, and the patient is caught in between, this is what you get.
----------------------
8/2/2025, “German
nursing homes see cost for care explode,” by Volker Witting, DW
Quote: “The cost of a
stay in a nursing home has risen to an average of €3,248 ($3,760) per
month, according to the German Association of Nursing Homes (vdek), an
association that represents the interests of several statutory health
insurance providers.”
LTC Comment: We warned over 20 years ago that Germany’s LTC
“insurance” plan would not be the end all and be all it was being made out
to be:
LTCI in Germany and
Don't Look to Germany for a Long-Term Care Model. Now reality is
setting as it is about to do for our Social Security and Medicare
entitlements. At least we dodged the LTC entitlement trap … well, except
in Washington State. ***
LTC BULLET: LTC MUSINGS
LTC Comment: I used to think long-term care was
pretty simple and straight forward … both the problem and the solution.
People become old, injured, or demented and they need
help with activities of daily living. That help can be very expensive.
But, like death, age and disability are things people
don’t like to think about, so they tend not to plan for them.
Consequently, many people end in need of LTC but
unable to pay for it.
So, government wanted to help. Medicaid came along 60
years ago this month and started paying for nursing homes, the main care
venue available at the time.
Two big things happened quickly:
-
Medicaid LTC costs exploded because nearly everyone
qualified.
-
The public stopped worrying about LTC because
government paid.
Policymakers and politicians adapted by making
Medicaid LTC harder to get with asset transfer restrictions and other
eligibility controls.
But lawyers specializing in “elder law” found ways
around Medicaid’s eligibility restrictions, making their affluent clients
as quickly and easily eligible as the poor, often more so, by streamlining
and systemizing the application process.
When I started working on the LTC issue in 1982, this
was the situation.
Most people ignored LTC until they needed it. The
poor qualified for Medicaid care. The middle class and affluent did as
well, often with help from specialized “Medicaid planners.”
I figured that as long as the public could ignore LTC
risk and cost, wait to see if they ever need extended care, and get the
government to pay if they do, why would they plan, save, invest or insure
for LTC?
Specifically, I noticed there was a budding new
product, called private LTC insurance, trying to get a foothold in the
market. How I wondered would it have a chance competing with Medicaid?
To buy insurance for a risk, people have to believe a
risk exists and plan ahead. But everything about government’s handling of
LTC sent the message: “don’t worry, if you ever need LTC, Medicaid will
pay.”
As I studied the issue I concluded “you can’t have it
both ways.” You can’t provide free LTC after the insurable event occurs
through Medicaid and still expect people to buy private insurance for LTC
risk with high premiums 30 years in advance.
So I did a study and wrote a report in 1985 for the
Health Care Financing Administration (CMS’s predecessor) advocating that
if Medicaid is to pay for LTC when needed it should also secure exempt
property so it isn’t transferred to qualify and require recovery from
recipients’ estates when the wealth is no longer needed by qualified
relatives.
That way, people would have skin in the game. They
would figure “if I ever need LTC, Medicaid will pay, but Medicaid is
welfare with a poor reputation for access and quality, and if I rely on it
I’ll have to pay it back out of my estate anyway, so maybe I should
consider this new LTC insurance product. You can still read that
40-year-old report
here.
HCFA suppressed that report, believing Regional
Office staff should not be writing and publicizing national policy
studies. But the USDHHS Inspector General and the Government
Accountability Office picked it up and did similar studies under their
imprimaturs. The IG hired me out of HCFA to do its study and write its
report, published in 1988 and available
here.
The LTC social contract described in that study
became law in the Omnibus Budget Reconciliation Act of 1993. Most of the
study’s recommendations, such as longer and stronger transfer of assets
restrictions and mandatory estate recoveries, became statutory
requirements for state Medicaid programs to impose.
Had the new rules been implemented and enforced,
planning for LTC by saving, investing or insuring would have become
routine as a sensible way to avoid dependency on Medicaid with its welfare
stigma and poor quality, combined with the requirement to pay it back from
the estate.
Instead of incentivizing adult children to save their
inheritances by putting their ailing parents on Medicaid, the new system
would encourage them to help their elders pay privately for LTC and stay
off Medicaid with its various downsides. It would also encourage the
younger generation to prepare for their own future LTC need.
But as it turned out, states did not implement the
new rules effectively; the federal government did not enforce the rules;
the media didn’t publicize them and consumer behavior did not change.
As a consequence, we find ourselves decades later
with Medicaid LTC costs continuing to soar, with access and quality
deficient, with private LTC insurance languishing, and with little hope
for improvement.
What’s worse, there have been recent calls to cut
back or eliminate mandatory estate recovery, limiting or removing one of
the only provisions in the rules to encourage early LTC planning.
Whereas Medicaid LTC eligibility was always easy to
obtain, especially with legal assistance, it has become easier than ever
due to the widespread practice of artificially spending down countable
wealth by using it to purchase exempt resources. See “Medicaid’s
$100+ Billion Leak” for details on that practice.
America’s faltering LTC system sinks deeper and
deeper into dysfunction. Nursing home bankruptcies are up. Assisted living
facilities follow nursing homes down
Medicaid’s primrose path. Realignment from institutional to home and
community-based care, expected to save money, actually drives up total
costs because those in home care need nursing homes eventually too.
Crazy, contradictory public policies encourage asset
accumulation on the one hand (Americans hold $97 trillion in home equity,
retirement savings and life insurance) but discourage asset expenditure
for LTC by Medicaid eligibility policy that allows high income and high
asset people to qualify easily while preserving wealth in exempt form.
The common assumption that Medicaid LTC eligibility
requires impoverishment is myth at best (misunderstanding), hoax at worst
(intentional). The common statement in popular and academic media that
millions of Americans are spending their life’s savings on LTC is
unsupported by facts. Only 6.5% of LTC expenditures could come from
savings.
LTC is not the high financial risk (70%?) it is often
reported to be. 55% who reach 65 will have no paid LTC costs. 31% will
need 2 years or less and 9 in 10 have resources (income and wealth) to
cover two years of assisted living. For the remaining 14% who need 2 years
or more, especially the 4% who need 5 years or more, Medicaid pays much of
the cost. Little wonder people worry so little about LTC until they need
it.
Estimates of out-of-pocket LTC expenditures are
dubious because they are based on
micro-simulations that assume people are paying going rates for care.
There is no evidence that people actually spend down savings for care as
opposed to reconfiguring wealth to qualify by other means, such as asset
transfers, irrevocable trusts, Medicaid-friendly annuities or purchase of
exempt assets.
Medicaid pays LTC providers notoriously low
reimbursement rates which accounts for the access and quality problems and
the caregiver shortages. Medicaid requires recipients to contribute most
of their income to offset the cost of their care to Medicaid. This in
effect converts what would have been private pay revenue at market rates
into Medicaid-level reimbursement that is a cause of many problems.
America’s dismally inadequate LTC system will not
improve until Medicaid pays market rates. Medicaid can’t pay market rates
until it covers fewer middle class and affluent people.
Medicaid treats the affluent well but crushes the
poor. Key money allows affluent people who have used Medicaid financial
eligibility loopholes to quality to access the best care to the exclusion
of the aged, poor and vulnerable Medicaid supposedly helps first.
So, in conclusion, America’s Medicaid-based LTC
system is much more complicated than it seemed when I first assessed the
situation in 1982. We made progress in 1993 with stronger asset transfer
limits and mandatory estate recovery. In the Deficit Reduction Act of 2005
we finally got the first ever cap on home equity. But since then, no
progress, and some back sliding.
I remain optimistic that the country will come to its
senses. Winston Churchill famously said “You can always count on Americans
to do the right thing - after they’ve tried everything else.” But I’m
convinced now that we will have to hit a financial wall before the right
corrective actions are taken.
When the country has borrowed so much and the rest of
the world loses confidence in our ability to service our debt, a reckoning
will occur. I expect that to happen in the 2030s when a triple threat
occurs. Boomers start turning 85 in 2031, Social Security and Medicare cut
back by mid-decade, and their reductions in support for Medicaid LTC will
spell the end of that program’s availability to middle-class and affluent
people.
At that point, by default if not by intentional
policy, Medicaid will shrink to a safety net for the poor, be forced to
pay market rates for care to attract enough caregivers, and become a much
better program for those in need when it no longer covers those who
should, could and would pay their own way going forward.
To make sense of what ails LTC, read the
Paragon Health Institute’s “Long-Term
Care: The Problem” and “Long-Term
Care: The Solution” and watch this “virtual
LTC event” featuring age wave visionary Ken Dychtwald and leading LTC
researchers. To find ample private funds for LTC, check out “Medicaid’s
$100+ Billion Leak.” For what not to do, see “Medi-Cal-amity:
California’s Reckless Expansion of Medicaid Long-Term Care to the Affluent.”
Much more on long-term care
here.
#############################
Updated Monday, August 4, 2025, 10:03
AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-028:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
German nursing homes see cost for care
explode
-
Genworth Gets More Approvals for Long-Term
Care Market Return
-
Study reveals how medication side effects
can lead to dangerous medication cycles in adults 65+
-
Federal funding cuts force retirement
research centers to close
-
Shield Your Assets as Part of a
Comprehensive Long-Term Care Plan
-
Where and How to Invest Your Long-Term-Care
‘Bucket’
-
Medicare Advantage in 2025: Enrollment
Update and Key Trends
-
First-of-its-kind study finds that
lifestyle programs improve cognition in older adults
-
Users of Medicaid HCBS increased while
users of institutional LTSS decreased from 2019 to 2021, new report
reveals
-
The number of family caregivers is surging
-
Long-term care insurance still a rare
benefit for employees, and enrollment is low
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Monday, July 28, 2025, 10:03
AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-027:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Why So Many Seniors Can’t Afford Long-Term
Care
-
Victims of Biden’s Enrollment-At-Any-Cost
Exchange Strategy
-
‘Gray Divorce’ Trend Threatens Retirement
Security
-
LTCi environment ripe for innovation
-
Does Using Medicaid Affect Quality of Care
in Long-Term Care Facilities?
-
Fiscal Fallout: Long-term care spending
driver of Washington DSHS’s swelling budget
-
Seniors face widening care gaps after
dementia diagnoses, major study reveals
-
CMS Finds 2.8 Million Americans Potentially
Enrolled in Two or More Medicaid/ACA Exchange Plans
-
Unpaid caregivers sacrifice more than
$15.5K annually, study finds
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Friday, July 25, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC BULLET: HAGELMAN REFLECTS
LTC Comment: Ron Hagelman has been an oracle of LTC
insurance knowledge for decades. Here he shares some off-the-cuff comments
on the business, its practitioners, and their beneficiaries, after the
***news.***
***
CLTCR Premium Membership -- Center for Long-Term Care Reform premium
members receive our full suite of individual membership benefits
including:
·
All LTC Bullets and E-Alerts
·
Access to our Members-Only Zone website and Almanac of
Long-Term Care
·
Subscription to our Clipping Service
·
Email/phone access to Steve Moses for 24-hour turnaround
queries
Our Premium Membership is designed to give you a competitive advantage
in your long-term care profession. Your increased knowledge of the
critical issues and challenges we face in the field of long-term care
service delivery and financing equals improved professional success for
you and better LTC services for your clients and for those who have no
choice but to rely on scarce public resources.
Stay on the forefront of professional knowledge and
help us fight for rational long-term care policy reform by contacting
Damon at 206-283-7036 /
damon@centerltc.com to start your Premium Membership immediately or go
directly to our secure online subscription page and
sign up for as little as $21 per month. ***
LTC BULLET: HAGELMAN REFLECTS
LTC Comment: You’ve read his columns in Broker
World and heard his formal presentations and casual comments at
long-term care meetings. Now peel away the formality and consider these
“personal reflections” straight from Ron’s heart.
“The Personal Reflections of a Veteran LTCI
Evangelist”
by
Ronald R. Hagelman, Jr. CLTC, CSA, LTCP
I have considered myself an insurance professional
for 40 plus years, three-fourths of it in LTCI and I will not give up the
notion that the good guys and girls in our chosen corner of the insurance
marketing universe are the ones that survive to tell their stories. We are
consistent in strapping on our fiduciary armor every morning to restore
and confirm each day our belief in the wisdom of understanding and
leveraging risk. We understand better than most the value of planning
ahead and drastically altering future outcomes by our diligent and caring
interference.
My insurance career seems to have paralleled the rise
of a new vital product and sales genre. I grew up in an insurance family.
As a product and distribution consultant uphill sales battles, innovative
product development and national marketing strategies have continued to
define my work, good and bad. In the 1980’s supplemental health plans
proliferated from cancer indemnity to nursing home supplements. These
augmenting policies and concepts helped create a rich sales environment
that fed a growing inventory of benefit added on and specific indemnity
enhancements. The industry did not ignore the risk. We simply had yet to
understand its actual size and benefit trajectory.
Our clients responded better to the idea of care at
home. With the advent of HIPAA, a corollary universe of senior home care
service companies also began to evolve. The government had taken drastic
action to incentivize the private market by defining a tax-qualified
comprehensive policy, fair benefit triggers and aggressive corporate
premium deductibility. New sales and the necessity of senior care support
at home began to flourish in tandem. In truth many of the readers of this
column just like me would never be the same. Subsequently, adverse pricing
adjustments, the Pension Protection Act expanding combo life and annuity
product options, partnership plans, NAIC rider restructuring and rate
stabilization have expanded our opportunities to sell protection into
place.
The new definition of the LTCI conundrum is no longer
only focused on sales and it is about to be overwhelmingly about claims.
The billions of claim reserve dollars we stockpiled so diligently into
place for the last 25 years should again caution us to follow the money
pouring through claim management. We must not forget the delay of payment
fines not so long ago levied against disability income carriers. Boomers
we worked so hard to prepare will begin to turn 80 next year when the
average age at claim is 78 and half will need care. We remain woefully
unprepared: reserves under pressure, claim management TPA’s who exclude or
diminish the role of professional financial planners in the claim process,
serious shortages of available caregivers and the persistent lack of will
from public or private sources to prepare for the claim tsunami now
rapidly approaching the beach.
I must strongly caution my fellow veterans, those who
care ahead and plan ahead to get your fiduciary claim support duck
parameters in a row. This is when Noah started looking for timber. I would
strongly recommend being prepared by establishing a relationship with a
senior care company that understands the complexity of LTCI and can help
expedite claims when the impact occurs. It is imperative we acknowledge
the volume of claims gathering just offshore. It is mandatory that we
applaud and gratefully recognize those agents who are now ready to hand
out safety vests to their past clients and righteously help their children
purchase their own future safety devices.
Ronald R. Hagelman has 44 years in the business,
currently consults for Amada Senior Care, received the ILTCI Recognition
Award (2024), and published over 250 LTCI articles. He created and
distributed over 50 Life, Health and Annuity products for 16 companies.
#############################
Updated Monday, July 21, 2025, 10:03
AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-026:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Respite care more than doubles chances of elderly
patients dying at home, study finds
-
Estate recovery is fair — if Medicaid is for the
needy
-
Nurse practitioners critical in treating older
adults as ranks of geriatricians shrink
-
Genworth's CareScout Unit Unveils Long-Term Care
Insurance Strategy
-
Caring for a loved one with dementia is hard.
Financial planning can alleviate the stress.
-
Estate, Long-Term Care Plans Under the ‘Big
Beautiful Bill’
-
‘I enjoy vacations to Europe’: I’m 75 and have $1
million in an IRA. Why do I feel guilty?
-
Retirement conditions more challenging for late
baby boomers, later generations
-
Your Guide to Medicare Dual Eligible Special Needs
Plans (D-SNPs)
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Monday, July 14, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC E-ALERT #25-025:
LTC NEWS AND COMMENT
LTC Comment: Do you spend hours searching
the internet for useful articles, key data, and relevant reports to keep
you on the forefront of professional knowledge? Do you lose business
because you’re blindsided by clients or competitors who learn critical
information before you do? Here’s an antidote:
LTC Clippings: The Center for Long-Term
Care Reform notifies subscribers to our LTC Clippings service daily of
information you need to know. Each message contains only the critical
facts about new publications: a title, representative quote, a link to
the original, and our analysis in a sentence or two. To inquire or
subscribe, contact Damon at 206-283-7036 or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC E-Alerts: Once a week, we compile our
daily LTC Clippings into a summary, email it to Center for Long-Term Care
Reform members, and archive it in The Zone, our password-protected
members-only website. Center members also receive our weekly LTC Bullet
op-ed. To join the Center and receive all these benefits and more,
contact Damon at 206-283-7036 or
damon@centerltc.com.
We no longer post our LTC E-Alerts on the
Center’s public access website, but here’s what today’s LTC E-Alert
contained: links, quotes and comments on the following articles, reports,
or data:
-
Hospital-to-home
transitions fail seniors with dementia and multiple conditions, study
reveals
-
UPDATED: Genesis
HealthCare files for bankruptcy, nearing sale
-
The Number Of
Americans Planning To Leave An Inheritance Goes Up As The Number
Expecting To Receive One Goes Down
-
Be inspired by
this feature article on Maddy Dychtwald's work and life
-
Labor Department
withdraws Biden-era proposal to eliminate subminimum wages for disabled
workers
-
New Trump budget
‘a significant win’ for providers; optimism among the gloom
-
New York releases
Master Plan for Aging providing 100 aging-in-place solutions
-
Changes made — and
not made — to WA Cares in 2025
#############################
"LTC E-Alerts" are
a
feature offered by the Center for Long-Term Care Reform, Inc. to members
at the $150 per year level or higher. We'll track and report to you news
and analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Monday, July 11, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC
BULLET: MEDICAID OVERSIGHT
LTC
Comment: Medicaid should help the poor, but crushes them. The affluent
should pay for their own LTC, but don’t. Then they take the best Medicaid
offers. What’s wrong and what to do? After the ***news.***
***
LTC PROVIDERS struggle to provide decent LTC while Medicaid pays too
little to meet that minimal standard. Now the federal government wants to
cut back even more. Fighting to keep the already inadequate status quo is
not the answer. It’s high time to fight back. So I wrote this column for
McKnight’s LTC News suggesting how the LTC profession should
proceed. Check it out and let me know what you think: “The
best defense is a good offense,”
***
LTC
BULLET: MEDICAID OVERSIGHT
LTC
Comment: We had a chance to address the inequities in Medicaid LTC with
the “One Big Beautiful Bill.” But that opportunity passed. What should we
do now? Here’s one way to save billions and improve Medicaid for those who
need it most.
“Medicaid Oversight”
by
Stephen A. Moses
Medicaid is the talk of the town. Republicans want to “fix” it (reduce
costs). Democrats want to “save” it (no change). But Medicaid’s biggest
component and its dirty little secret go unaddressed.
Medicaid funds
61
percent
of long-term care (LTC) in the USA and LTC consumes
37
percent
of state and federal Medicaid spending. But only
six
percent
of Medicaid recipients use LTC and spending on them is
nine
times higher
than for non-LTC users. So LTC overweighs Medicaid spending.
Yet
the big funding debate just concluded in Washington, DC ignored LTC.
Advocates and opponents of the One Big Beautiful Bill (OBBB) fought over
the 63 percent of Medicaid dollars that go to the other 94 percent of
recipients. That’s important of course, but it should not have excluded
LTC.
What
about LTC should analysts and lawmakers consider more closely? The three
things everyone knows about LTC are that
-
most people will need it as they age;
-
LTC is very expensive; and
-
it
wipes out the life’s savings of millions of Americans.
But
Mark Twain said “It ain't what you don't know that gets you into trouble.
It's what you know for sure that just ain't so.” That adage applies
perfectly to Medicaid and LTC.
Which things most people think they know about LTC are not so? And how
should that information become part of the mission to improve Medicaid
while reducing its cost?
LTC
wipes out the savings of millions of Americans?
Not so. Only 12.9% of LTC spending comes out of people’s pockets and half
of that is income (mostly from Social Security) that people already on
Medicaid have to pay to offset the cost of their care. Only $1 in $15
(6.5%) could come from savings. There is no evidence of widespread
catastrophic LTC spend down, only anecdotes.
Medicaid LTC eligibility requires low income?
Not so. Medicaid either deducts private health care costs from income
before applying a limit or it allows income diversion trusts. So,
high-income applicants with commensurately high private expenses qualify
routinely.
Medicaid LTC eligibility requires low assets?
Not so. Most large assets seniors own, such as home equity, retirement
savings, one business, a vehicle, personal belongings,
and
others,
are exempt from the asset test. Mandatory estate recovery is only lightly
enforced and easily avoided.
Countable assets, such as cash, stocks, bonds, etc., over $2,000 preclude
Medicaid LTC eligibility?
Not so. Countable assets are easily reduced or eliminated entirely by
using them to purchase exempt resources, a common technique explained in “Medicaid’s
$100+ Billion Leak.”
Medicaid LTC eligibility serves the poor, aged and disabled best?
Not so. Medicaid income and asset spend down rules quickly crush the needy
who have few resources and little advice from financial advisors on how to
qualify for Medicaid without devastating financial consequences.
All
Medicaid recipients receive the same care?
Not so. Poor, aged and disabled recipients tend to live in neighborhoods
with nursing homes and other LTC providers that are most heavily dependent
on Medicaid’s low reimbursement rates resulting in deficient access and
quality.
Middle class and affluent people would never seek Medicaid LTC eligibility
due to its poor reputation for access and quality?
Not so. The well-to-do who self-impoverish artificially hold back “key
money” to pay privately before they convert to Medicaid. This ensures
their access to the best nursing homes and other LTC providers that are
desperate to attract private payers at much higher rates than Medicaid
pays. Once in, they can’t be removed when their payment source changes.
Medicaid’s dirty little LTC secret is that it punishes the poor and
rewards the affluent leaving the latter with little reason to worry about
LTC risk and cost. This is why few plan for LTC and most end up on
Medicaid when care costs escalate beyond their incomes.
Is
there one thing the Congress could do that would save money and reduce
this inequity?
Yes.
Apply the same rule to asset spend down that already applies to income.
High-income people qualify for Medicaid LTC, but only after they prove
they spent down for actual medical or LTC expenses. High-asset people,
however, are under no such obligation to spend down for care. They can
spend excess countable assets to purchase exempt resources, becoming
eligible while hiding their wealth for heirs to inherit.
This
oversight in Medicaid LTC financial eligibility rules lets the affluent
take the best of what Medicaid offers and leaves fewer resources in the
program to serve its more appropriate, needier recipients. It also creates
a moral hazard by eliminating the need for people to plan early for LTC by
saving, investing, or insuring against the risk.
Solution?
Require that Medicaid LTC asset spend down be for private medical or LTC
expenses, not just to buy exempt assets. Based on a
2014
Government Accountability Office report,
we estimate this could
save
Medicaid $100 billion or more
every two or three years as burgeoning numbers of elders move through the
LTC financing system.
Confronting LTC’s realities instead of accepting its commonplace fallacies
is a foolproof way to save money and improve Medicaid for the vulnerable
people who need it most.
#############################
Updated Monday, July 7, 2025, 10:03
AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-024:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
The One Big Beautiful Bill
Now Heads to President Trump
-
Feds ensnare home-based care
providers in nationwide healthcare fraud crackdown
-
Don't Rely on Medicare or
Medicaid for Your Long-Term Care
-
Senate Passes Bill Keeping
Helpful Nursing Home Provisions Intact But Worries Remain
-
Older childless Americans
worry about who'll care for them — do these 4 things if you’re 50-plus
with no kids
-
The best defense is a good
offense
-
CMS proposes 6.4 percent home
health rate cut for 2026
-
The Senate Improves OBBB's
Health Policy Provisions
-
A Perfect Storm Is Poised to
Raise Long-Term Care Costs. Here’s How You Can Get Ahead of It
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Monday, June 30, 2025, 10:03
AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-023:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Discrepancy exists between proposed federal
budget, what Americans want, survey finds
-
Documentary pulls back curtain on home care
-
US Short-Term Care Insurance Market to Grow
from USD 45 Billion to USD 110.1 Billion by 2033 with a Robust 10.2%
CAGR
-
More Boomers Can Afford Senior Living, But
Development Shortfall Threatens ‘Severe Shortage’ Ahead
-
10 Warnings Clients Would Give Their
Younger Selves About Long-Term Care
-
Rogers Victor: America’s senior health
crisis needs fresh solutions
-
National Health Expenditure Projections,
2024–33: Despite Insurance Coverage Declines, Health To Grow As Share Of
GDP
-
Financial strain, illness hinder seniors’
desire to age in place, CenterWell survey finds
-
California budget must consider growing
older adult population
-
UPDATED: Providers ‘hopeful’ but
‘skeptical’ as feds announce insurers, MA plans will limit prior
authorization use
-
CAPITAL IDEAS: Should millionaires buy
long-term care insurance?
-
If You Want Medicaid to Cover Long-Term
Care, Get Ready to Hire a Lawyer
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Monday, June 23, 2025, 10:03
AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-022:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
#############################
-
New dashboard breaks down by state, county
the number of people using Medicaid HCBS
-
1 trillion in cuts to Medicaid would have a
devastating impact on people receiving long-term care. Here's why
-
Why is caregiving so hard in America? The
answers emerge in a new film
-
Higher Medicaid mix drives down nurse
staffing, regardless of ownership type
-
MA plans extend hospital stays, reduce
post-acute services
-
Medicare and Social Security go-broke dates
pushed up due to rising health care costs, new SSA law
-
Older adults in the US are increasingly
dying from unintentional falls
-
States allocate highest percentage of
revenue to Medicaid in FY 2023 in 20 years: report
-
New study reveals seniors are money-savvy
until dementia sets in
-
Senior care insurance costs double over a
decade with steepest risks for SNFs
-
Study projects Alzheimer’s financial burden
will hit African American and Latino families hardest by 206
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Monday, June 20, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC
BULLET: MEDICAID’S LONG CON
LTC
Comment: How did Medicaid swindle LTC providers, insurers, and consumers
for six decades? Answers after the ***news.***
|
*** TODAY'S LTC BULLET is sponsored by Claude
Thau (BackNine Insurance). BackNine gives you a free
personalized website at no cost. Your clients (& family & friends)
can, with as little or as much of your involvement as you or they
want, buy life insurance and LTCi, and can speed issue by scheduling a
paramed and uploading medical records immediately. We quote
stand-alone LTCi, linked-benefit and life with a LTC rider
side-by-side. Claude is the lead author of Milliman’s annual Broker
World LTCi Survey & a past Chair of the Center for Long-Term Care
Financing. Contact him at 913-707-8863 or
claude@back9ins.com to learn about more
great BackNine features and services. *** |
***
PARAGON ON THE OBBB: As we enter the dog days of summer, weighty questions
are under consideration in Washington, DC and consequential decisions will
soon be made. The Trump administration’s One Big Beautiful Bill (OBBB)
touches health policy and LTC policy in significant ways. For the health
policy issues at stake, follow the
Paragon Health Institute’s
many
reports,
articles
and
weekly newsletter.
On the LTC side, stay tuned here. LTC providers worry caps on provider
taxes in the OBBB will hurt state Medicaid programs and reduce providers’
already inadequate revenue stream. But I think “The Best Defense is a Good
Offense” so I’m hoping McKnights LTC News will publish my draft
article of that title. It proposes an amendment to the OBBB that would
save the billions of dollars Republicans seek while delivering the better
access to higher quality care Democrats demand. ***
LTC
BULLET: MEDICAID’S LONG CON
LTC
Comment: The more I thought about the history of Medicaid’s role in
providing and funding long-term care, the more it seemed like a
decades-long confidence game. Promising to help the poor with LTC, the
program instead captured LTC providers between the rock of inadequate
reimbursement and the hard place of mandatory quality. Medicaid tricked
insurers into offering a product the program was giving away to the same
middle class and affluent people who should have bought it. And consumers,
barraged with warnings that LTC could wipe out their life’s savings, were
duped into complacency by the reality that when the time came, late in
life, that they faced potentially catastrophic LTC costs, Medicaid always
paid. The consequences couldn’t be more real if they were intentionally
inflicted by a bad actor rather than the haphazard result of centrally
planned, government regulated, interference in the LTC marketplace.
So,
I started writing. The following essay is a work in progress. There is
much to change and more to add before it is complete. So take it with a
grain of salt for now. And think about what a mess Medicaid has made of
LTC service delivery and financing.
“Medicaid’s Long Con”
by
Stephen A. Moses
A "long
con"
is a “sophisticated and extended confidence game where a swindler slowly
gains the victim's trust over a long period to eventually extract a large
sum of money or other valuable assets. It involves multiple stages and
careful manipulation of the victim's perception to make them believe they
are in control while being subtly guided towards the con artist's desired
outcome.”
That
definition, culled from AI, brings to mind how Medicaid, the dominant
payer for long-term care (LTC) in the USA, has duped LTC providers,
insurers, and consumers into making poor financial decisions and accepting
insufferable economic conditions. From this perspective, let’s review each
LTC player’s relationship with Medicaid one at a time.
Providers
Starting with its passage in 1965, Medicaid sold LTC providers (almost
exclusively nursing homes at the time) a bill of goods. Reimbursements
were generous at the start. With no asset transfer restrictions or estate
recoveries in the beginning, new Medicaid admissions soared. Nursing homes
evolved from largely Mom and Pop operations into a vast industry of big
corporations maximizing revenue from the public welfare program. As
Medicaid paid exclusively for nursing home care, other potential modes of
service delivery, such as home care or assisted living, were stymied for
decades.
This
sweet deal for nursing homes didn’t last long. Medicaid LTC expenditures
exploded from the start. To control costs, state Medicaid programs reduced
reimbursement levels. To compensate, nursing homes charged private payers
more. Private payers responded by seeking Medicaid eligibility, often
facilitated by Medicaid planning attorneys exploiting financial
eligibility “loopholes.” Nursing homes’ private-pay revenue collapsed from
half in 1970 to under ten percent in 2023. In the meantime, many state
Medicaid programs established certificate of need programs to limit
construction of new nursing homes on the principle that “they can’t charge
us for a bed that doesn’t exist.” But this practice gave existing nursing
homes a de facto monopoly by excluding potential competition, further
undercutting the incentive to provide quality care.
Over
time Medicaid nursing home reimbursements became so inadequate that access
and quality deteriorated substantially. Media exposés of awful
institutional conditions proliferated. National legislation passed in 1987
requiring better care, but little changed. It became so bad that new
venues and modes of care finally became available, because, faced with the
choice between nursing home care paid for by Medicaid or the new and
rapidly growing option of assisted living, financially able consumers
chose to pay privately for the more desirable alternatives. In time,
private-pay home care also got traction as consumers’ distaste for
Medicaid funded nursing home care grew.
How
does this history display the trappings of a swindle? Nursing homes were
led down a primrose path to rely almost exclusively on Medicaid (and some
Medicare) financing. Their private pay revenue stream, half again as much
as Medicaid pays, nearly disappeared as savvy consumers took advantage of
the easily available public financing. As care quality deteriorated and
consumers migrated to other private-pay options, nursing homes were left
with too little revenue to hire and retain enough caregivers resulting in
further deterioration of care access and quality. Nursing homes and other
Medicaid LTC providers don’t even get the benefit of the relatively low
out-of-pocket LTC spending that consumers still pay (12.9 percent of total
LTC spending). Medicaid converts recipients’ private income and asset
spend down into its egregiously low level by requiring recipients to pay
most of their income (largely Social Security) to the LTC provider to
offset the cost to Medicaid.
If a
con artist had set out in 1965 to trap LTC providers in a system that
disables their ability to provide quality care while holding them
accountable to achieve unrealistic standards, he could not have done a
more effective job than Medicaid itself has done, however haphazardly.
Insurers
How
did Medicaid ensnare insurers? When Medicaid LTC expenditures exploded in
the early 1970s, lawmakers and program officials started clamping down.
Transfer of assets restrictions and estate recoveries were first
authorized (TEFRA ’82) and later made mandatory (OBRA ’93). In 1988, the
DHHS Office of Inspector General published a
report
(full disclosure, I wrote it) that said in paraphrase: if we’re going to
let people get Medicaid LTC benefits while retaining large exempt assets,
then they should have to pay it back out of their estates. That was the
quid pro quo in OBRA ’93.
So
the OBRA ’93 message to insurers was: Medicaid will no longer pay all the
LTC costs for everyone. People now have to pay their own way until they
qualify under Medicaid’s stringent income and asset rules … or … they’ll
have to pay back everything Medicaid pays for their care out of their
estates. More distressing yet, most analysts and the media went even
further. They insisted people could get no help from Medicaid until they
spent down all their savings into impoverishment. Some big insurance
companies took this draconian LTC situation to the bank, or so they
thought.
Starting in the 1980s and through the early 2000s, over 100 insurance
companies made private LTC coverage available. They priced it low to
attract market share and because solid historical actuarial data on the
incidence of paid LTC was unavailable to counsel them otherwise. Who
wouldn’t buy this coverage, they speculated, given the consequences of
going bare: total impoverishment or loss for heirs of the estate to
Medicaid recovery? But results did not meet expectations. It turned out
that prospects for the coverage didn’t buy the hype about total economic
risk; the estate recovery liability was never fully enforced or
publicized; and the public remained too complacent about LTC risk and cost
to purchase the expensive LTC coverage.
Medicaid duped the private insurance industry into thinking LTC was a big
financial risk that people would buy coverage for and then pulled the rug
out from under the carriers who tried, by making catastrophic coverage
available even to the middle class and affluent after the insurable event
occurred. The end result is that relatively few people plan and insure for
LTC and most end up on Medicaid if they need high cost extended care.
Swindled by Medicaid’s bait and switch, the LTC insurance business has
evolved creatively and maintained a foothold but it has now, and can only
anticipate for the foreseeable future, a relatively minor role in
financing LTC.
Consumers
Perhaps the biggest losers in Medicaid’s long con are consumers,
especially the needy whom the program is supposed to serve. The public was
trapped in a welfare-financed LTC system for decades that gave them
nothing but nursing home care. Only after that system deteriorated to the
point of a national disgrace, did enough financially able consumers rebel
by spending their own money for newly evolving private home and
community-based care options. But LTC is so long in duration and so
expensive to pay for privately, families were put in the position of
having to care for their own loved ones as long as possible. This caused
tremendous financial and emotional stress, leading them to turn to
Medicaid when the strain and cost became too much.
That’s when Medicaid softens the blow. Despite conventional wisdom,
drummed into everyone by the media (remember “Dying
Broke”),
that Medicaid LTC requires spend down for care into impoverishment, the
reality is very different. Middle class and affluent people, once they
consider and look into public financing options, find that eligibility for
Medicaid is relatively easy. Income is no obstacle for people with high
private medical or LTC costs because those costs are deducted before a low
income standard is applied. Likewise, high assets don’t matter as they are
either already tied up in exempt resources (the home, retirement savings,
a vehicle, person belongings, etc.) or they’re easily converted to exempt
status by using countable assets to purchase non-countable resources. See
“Medicaid’s
$100+ Billion Leak.”
Here’s the irony and the tragedy. Medicaid financial eligibility rules
crush the poor quickly. They lack resources to pay privately even for a
while. They end up in the worst nursing homes and LTC providers, the ones
that are heavily dependent on Medicaid’s low reimbursements. So the people
Medicaid is supposed to serve first, the aged, disabled, and
disadvantaged, get the worst care Medicaid provides. But what about those
middle class and affluent people Medicaid allows to qualify so easily?
They hold back enough “key money” from their artificial
self-impoverishment process, so they can pay privately for a few months.
That gives them access to the nursing homes and LTC providers, who have
relatively few Medicaid recipients, and are less dependent on Medicaid’s
poor reimbursements. They crowd out the poor and most needy from the best
care.
So
here’s how Medicaid swindled consumers. By making Medicaid LTC benefits
easy to obtain late in life after the insurable LTC event occurs, Medicaid
created a moral hazard. The public doesn’t believe the scare tactics
insisting that LTC is a catastrophic risk. People don’t know who pays for
LTC, but they can see someone must. Alzheimer’s patients aren’t dying in
the streets in large numbers. So consumers don’t worry about LTC until
they need it at catastrophic levels and then they slip seamlessly onto
Medicaid. By making the best care Medicaid offers available to people who
can afford to hold back “key money,” the program added insult to injury.
It helps most the very people who, if they bore more of the cost of LTC,
would protect themselves earlier with savings and insurance in order to
avoid the need to co-opt Medicaid’s scant resources.
Summary
Medicaid’s long con continues to this day. LTC providers, suckered by the
promise of practically unlimited customers and revenue, find themselves
struggling to supply decent care at less than the cost. LTC insurers
struggle to sell a product Medicaid has been giving away for 60 years,
with its best care going to the very people who should, could and would
have bought LTC insurance in Medicaid’s absence. Consumers, duped by
Medicaid to think they don’t need to worry about LTC when they are young,
healthy and affluent enough to prepare for the risk, end up dependent on a
deficient welfare program that does a better job for the financially able
than for the poor and disabled it was supposed to serve first.
Do
you think the confidence game analogy is inapt? No one set out to mess up
America’s LTC financing system so badly? Well, consider this: “Central
planning, public funding, heavy regulation, and easy access to welfare
benefits have caused most of LTC’s problems, such as nursing home bias,
poor access and quality, inadequate revenue for care providers, caregiver
shortages, and the terrible emotional and financial distress for
caregiving families. Medicaid especially is responsible because, despite
the conventional wisdom that it requires impoverishment, the program’s LTC
benefits are routinely available not only to the poor but to the middle
class and affluent as well.” (Source)
To say the terrible results were unintentional is a distinction without a
difference. The same causes always produce the same results.
#############################
Updated Monday, June 16, 2025, 10:03
AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-021:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
AMA Opposes Estate Recovery to Recoup Medicaid $$
From Dead Beneficiaries
-
More Americans Are Filing for Retirement Benefits
Earlier—Their Long-Term Retirement Security Could Suffer as a Result
-
More workers caring for aging parents than those
caring for preschool children, survey finds
-
More Americans aging into retirement are still
paying down mortgages
-
Study: 82 percent of unpaid caregivers suffer
mental health struggles
-
‘Consequences Are Undeniable’: New AHCA Survey
Warns Medicaid Cuts Could Force Nursing Home Closures
-
Your Company Needs an Eldercare Policy
-
Medi-Cal and Asset Tests: Hit by Reality
-
US dementia caregiving costs to surpass $3T by
2060, study indicates
-
Alzheimer’s Association launches free app for newly
diagnosed dementia patients
-
Family caregivers provide $873.5 billion in unpaid
labor annually: report
-
Gov. Newsom proposes ‘asset test’ for low-income
and disabled Medi-Cal applicants. What does that mean?
-
660,000 more LTC workers needed by 2030, skilled
nursing still below pre-pandemic levels
-
How Nondisabled Medicaid Recipients Without
Children Spend Their Time
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Monday, June 02, 2025, 10:03
AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-020:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Alzheimer’s Association launches free app for newly
diagnosed dementia patients
-
First Look: Understanding the Governor’s 2025-26
May Revision
-
Failure to factor in LTSS costs ‘most significant
risk’ to retirement income
-
How Medicare Advantage Changed Home Health Care Use
-
Health Care Provisions in the One Big Beautiful
Bill: Summary and Analysis
-
5 Key Facts About Nursing Facilities and Medicaid
-
AI predicts cognitive frailty risk in older adults
with 84 percent accuracy, study finds
-
The Middle-Class Dilemma: Funding Long-Term Care
Without Insurance
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Monday, May 30, 2025, 10:03
AM (Pacific)
Seattle—
#############################
LTC
BULLET: WHY SHOULD THE WEALTHY BUY LTCI?
LTC Comment: Why buy
insurance when you can afford to self-fund for the risk and cost of
long-term care? Answers after the ***news.***
*** WHO PAYS FOR LTC?
We’ve explained
elsewhere how little of the cost of LTC gets paid “out of pocket.”
Here’s a table summarizing all of the LTC financing sources.

Note that only 12.9% of
LTC spending comes out of pocket. But half of that is spend through of
income (not savings) that people already on Medicaid half to contribute to
offset Medicaid’s cost for their care. So, only about 6.5% of total LTC
expenditures could come from savings, despite all the media hullaballoo
about how LTC wipes out the life savings of millions of Americans.
That brings us to this
LTC Clipping we published last week about similar findings
presented by
Andrew Biggs of the
American Enterprise Institute.
5/20/2025, “No,
Long-Term Care Costs Aren’t Going to Cause a Retirement Crisis*,” by
Andrew G. Biggs, American Enterprise Institute
Quote: “*Unless we eliminate Medicaid, Medicare, state
programs, private insurance and charities. Then sure, we’ve got a problem.
… But assuming that retirees pay nothing for long-term care is actually
closer to the truth than Morningstar’s assumption that seniors pay 100% of
costs out of pocket, given that we know seniors actually only pay about
14%. This would be particularly true for lower-income seniors, where
long-term care costs almost certainly would be covered by Medicaid. For
instance, a 2022 analysis published
by the Department of Health and Human Services projected that 73% of
low-income seniors will pay nothing out of pocket for long-term care
services. The overall out-of-pocket average for this group is slightly
over $6,000. Not per year, but ever. In short, the Morningstar analysis
doesn’t point toward Americans facing a retirement crisis. If anything, it
indicates the opposite.”
LTC Comment: Finally another analyst (besides me) who gets it
right. Assuming that huge LTC costs will wipe out elders’ savings is just
wrong. Only 14% of LTC expenditures come out of pocket and half of that is
Social Security income people already on Medicaid have to contribute to
offset the program’s cost for their care. Only 7% could come from savings,
one dollar out of 14. Unless and until the USA puts more private wealth at
risk for LTC, most people will ignore LTC risk, end up on Medicaid without
spending down their savings for care, and suffer the poor LTC access and
quality the government provides. [Excuse the slight variances in
percentages as they come from using different data bases.] ***
LTC BULLET: WHY SHOULD
THE WEALTHY BUY LTCI
LTC Comment: “Let me
tell you about the very rich. They are different from you and me.”
F. Scott Fitzgerald
That sentiment holds
true for the reasons high net worth people should consider purchasing
private long-term care insurance. In today’s “Guest Bullet,” Center for
LTC Reform individual member
Shawn Britt of corporate-member
Nationwide explains why the wealthy would be well advised to buy LTCI.
The very rich may have different “pain points” than the less affluent.
Finding those vulnerabilities, identifying them, and asking the right
questions to bring them forward are keys to helping the wealthy see the
need to insure. Read Shawn’s cogent advice and apply it for your
well-to-do clients’ benefit … and yours.
"Why the Wealthy Shouldn't Overlook Long-Term Care Insurance"
by
Shawn Britt – CLU, CLTC
Long-term care insurance
is often thought of as a “safety-net” for the middle market, but in
reality, LTC coverage is for everyone! Too often, high net worth (HNW)
clients approaching their financial professional about purchasing LTC
coverage are told “you can afford to self-fund long-term care.” It happens
in reverse as well, with clients rebuffing a LTC discussion by saying “we
plan to self-insure.” However, being able to afford self-funding does not
make it a good idea. There are many sound reasons for the wealthy to use
LTC coverage in their financial strategy.
Find financial pain
point
How do you discuss the
need for LTC coverage with HNW clients in a way that makes sense? For
these clients, you are looking for their “financial pain point” – a
concern related to money that can be solved or protected by having LTC
coverage. Yes, they can afford to pay for their own care, but that
involves spending money – funds that may have been allocated to be used
for better purposes. When you find their financial pain point, you justify
the need for LTC coverage, particularly if that pain point has an
emotional tie to it. But first, it is important to understand just how
much the affluent and the HNW spend on long-term care expenses.
Highly affluent
individuals spend more on long-term care
High net worth and
highly affluent clients typically spend more on LTC than the typical upper
middle class or middle market client.
• The
HNW and highly affluent people are less likely to receive physical care
from their adult children – who are more likely to have
executive/professional level jobs
• The
HNW are more likely to stay at home for care, no matter the cost. The
current national average cost for 24/7 care at home exceeds $260,000
annually, but can run $350,000, $400,000 or higher in the wealthier
communties!1
• For
those going to a facility, it is often a top end “luxury” facility with
services and amenities not typically found in a traditional facility. The
cost of receiving care in such an atmosphere can run upwards to $35,000 a
month.2 That can add up to over $400,000 per year in today’s
dollars.
The cost of an LTC event
for a HNW or highly affluent individual that lasts three years can easily
exceed a $1,000,000 or more in today’s dollars - and fifteen to twenty
years from now, costs could run from $2 million to $4 million for an
individual or a couple. That is a lot of money – even for the wealthy!
When you discuss that level of cost with a client, the idea of
“self-insuring” may start to lose appeal. How could those same dollars
have been put to a better use if the HNW client had used cost effective
insurance to pay for their LTC expenses?
How LTC Insurance
Eases the “Financial Pain Points”
The following are just a
few of the potential pain points you may discover when talking with your
financially affluent and HNW clients.
• Ask
your client to list the charities and causes they would like their estate
to donate to upon their death. Then after showing them the cost of a
3-year LTC claim that could cost anywhere from $1 million to $2 million
(depending on when the claim commences), ask them which charity should be
crossed off the list.
• Is
your HNW client heavily invested in real estate or businesses that cannot
be easily liquidated? An LTC event taking place when this client is asset
rich and cash poor could result in having to sell an asset well below its
value.
• Does
your client have relatives or other people they are financially
responsible for? Using LTC coverage to fund those potential events make
much more sense than paying out of pocket.
• Does
your client call you every time the market takes a hit? Most clients,
regardless of wealth, do not want to see their account values go down.
Pulling out large amounts of money to pay for care in a down market
results in a double loss. The money cannot be grown back or grown forward.
• Self-funding
sets up the client’s estate to potentially pay unnecessary estate taxes.
If they are lucky enough not to need LTC, the “LTC funds” sitting in their
estate could be estate taxed. What if you could avoid that risk by using
the “self-insurance funds” to purchase LTC coverage at a faction of the
cost, and then donate the rest of the dollars to charity now, which would
allow for a tax deduction now? The tax deduction could help offset the
cost of the LTC insurance premium!
• Regardless
of wealth, putting one adult child in charge of a parent’s care puts them
in the position of making financial decisions that their siblings may not
agree with. Having LTC insurance helps take that issue off the table. When
LTC benefits are paying for the parent’s care, it is far less likely that
siblings will disagree on how the money is being spent, since the care is
being paid for by LTC benefits from an insurance company – not their
inheritance.
Final Thoughts
How do the HNW become
wealthy? Some inherit – but many build their wealth (or build it further)
by making good financial decisions throughout their life that include
leveraging assets and finding win-win solutions to potential problems. So,
why would they stop doing that now? The key is to find the pain point.
What really means something to the HNW or highly-affluent client that has
that has a dollar cost associated with it? Then show the client how
self-funding LTC expenses eats up the dollars they might otherwise devote
to that desire, such as charitable giving, liquidity needs, supporting
family members needing LTC, inheritances, major philanthropy or whatever
that pain point is.
Today’s LTC coverage
options attached to some form of financial product can offer guaranteed
premiums and benefits, and protect the investment in the policy from loss
if LTC is not needed. Long-term care coverage is just as important for the
HNW and highly affluent client as with any client – it is just for
different reasons.
Shawn Britt
is Director of Long-term Care Initiatives, Advanced Consulting Group,
Nationwide
1 A Place of
Mom – ”How Much Does 24/7 Home Care Cost in 2024? An In-Depth Guide” – May
9, 2024
2 Evelyn
Battaglia – Brick Underground “Where seniors can find luxury independent
living residences with resort-like amenities plus 24/7 personal care” –
August 22, 2023
#############################
Updated Tuesday, May 27, 2025, 10:03
AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-019:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Medicare vs. Medicaid for Long-Term Care: What You
Don't Know Can Cost You
-
Morningstar study on long-term care costs gets
pushback from think tank
-
No, Long-Term Care Costs Aren’t Going to Cause a
Retirement Crisis*
-
Explaining Waste, Fraud, and Abuse in Medicaid
-
Medicaid State Fact Sheets
-
10 Things You Should Never Say to a Caregiver
-
America’s retirement security hits ‘breaking point’
as Social Security funds dwindle: report
-
Federal judge sides with 23 states, blocks billions
in HHS cuts
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Monday, May 19, 2025, 10:03
AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-018:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Home health use remains high among beneficiaries
with dementia, study finds
-
Residents more likely to suffer physical
restraints, bedsores at bankrupt nursing homes: report
-
UnitedHealth under criminal investigation for
possible fraud in Medicare Advantage line: WSJ
-
Medicare ACO program shows no impact on end-of-life
care for dementia patients
-
Tracking the Medicaid Provisions in the 2025
Reconciliation Bill
-
Expanding state private insurance partnership
programs can help reduce public spending on long term care
-
Long-Term Care Provisions in the House Committee on
Energy and Commerce Bill
-
The Evergreen Model for Long-Term Care: A
state-level strategy for a persistent social policy problem
-
Caregiving: HHS Should Clarify When Youth May
Qualify for Support Services
-
“Here There Be Dragons”: The Myths and Claims
Undermining Medicaid
-
Congress Must Cut and Reform Medicaid
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Monday, May 16, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC
BULLET: UNDERSTANDING STRUCTURAL LONG-TERM CARE RACISM
LTC Comment: Is
Medicaid LTC set up to hurt the poor, underprivileged, and marginalized
while inordinately benefiting the affluent and middle class? Answers after
the ***news.***
*** GENWORTH/CARESCOUT
LTC SYMPOSIUM: On May 7, 2025 Genworth and CareScout convened a symposium
in Washington, DC on “Sustainable Solutions: The Future of Long-Term Care
Financing.” Read all about it on the program’s “landing page”
here. Genworth CEO Thomas McInerney welcomed the attendees.
Congressman Tom Suozzi, author of the WISH Act, keynoted the program. Four
panels followed focused on LTC financing policy and reform. I joined the
fourth panel, titled "Better Together..." – Public + Private
Collaboration, moderated by CareScout President and CEO Lynn White, along
with fellow panelists Stephanie Moench from Oliver Wyman and Susan Coronel
from AHIP. The end result of the half-day program was a long-sought, final
solution to the LTC financing crisis! Well, maybe not, but a sincere
effort toward that objective was made by all. Kudos to Genworth/CareScout
for underwriting and producing this program. ***
*** STOP THE PRESSES: I was just informed that a
“2025 Long-Term Care Symposium Recap” has been posted
here with this announcement: “On May 7, Genworth & CareScout hosted
our 2025 Long-Term Care Symposium. We convened leaders, advocates,
policymakers, and other stakeholders from the public and private sectors
to discuss how we can meaningfully progress toward solving our country’s
long-term care financing challenges. Take a look at the replays and photos from
the event, information about our panelists, supplementary videos
highlighting the perspectives of caregivers, and additional resources … .”
Check out panel #4, on which I served,
here. ***
LTC BULLET:
UNDERSTANDING STRUCTURAL LONG-TERM CARE RACISM
LTC Comment: A
couple years ago I began reading what has become a vast, peer-reviewed
literature about structural long-term care racism. Peer-reviewed articles,
many cited in the paper that follows, claim that underprivileged,
marginalized, often racial minority groups receive less and lower quality
long-term care than members of the more affluent demographic majority. The
authors make a compelling case for the discrepancies they identify. They
uniformly place the blame on Medicaid, especially that welfare program’s
deficient reimbursement rates that undercut access and quality. What they
fail to do, however, is to identify and explain the “laws, policies,
institutional practices, and entrenched norms” that disempower racial and
ethnic minorities and cause the care disparities they list. That is what
I’ve attempted to do in the following paper posted today to the
Center for LTC Reform’s website.
My paper
explains how Medicaid LTC financial eligibility policy affects the poor
and the affluent differently. It crushes the poor with stringent income
and asset spend down rules that impoverish them, often immediately. But it
treats the affluent and middle class very differently. They can have
virtually unlimited incomes as long as their health and LTC expenses are
high enough as they usually are for people who need expensive LTC. The
affluent can also retain virtually unlimited assets because seniors hold
most of their wealth in resources Medicaid considers exempt, such as home
equity. Even the very wealthy qualify for Medicaid by using special
trusts, annuities and other Medicaid planning techniques. Bottom line, the
affluent and middle class qualify for Medicaid LTC benefits almost as
easily and quickly as the poor.
But why would
the well-to-do choose Medicaid, with all its well-known deficiencies, when
they could afford quality care in the private market? The answer to that
question is the underlying cause of LTC racism. Prosperous people gain
access to the best care available from Medicaid. They are routinely
advised to hold back “key money” so they can pay privately for a while
before applying for Medicaid. This buys them access to the best nursing
homes and LTC providers who are desperate to attract private payers even
for short initial stays at 1.5 times the Medicaid reimbursement rate. The
poor and underprivileged, lacking any private funds after spending down
their meager incomes and assets to qualify for Medicaid, have access only
to the mostly Medicaid nursing homes and home care providers that receive
so much bad publicity about poor access and quality. The net effect is
that people with wealth receive the best Medicaid has to offer while the
less fortunate receive the worst.
That is the
root of structural LTC racism. Read the following paper for details and
see if you agree.
Title: Understanding
Structural Long-Term Care Racism
By: Stephen A. Moses
Abstract: Socioeconomically
marginalized groups, including racial minorities, receive lower quality
long-term care (LTC) in the U.S. compared to the more affluent majority.
Disparities include sub-standard nursing home care, impaired access to
assisted living or home care and reduced or inferior medical treatments.
Medicaid causes these deficiencies because it dominates LTC financing, but
pays too little to ensure quality. Many scholars conclude the system is
structurally racist. This paper examines the laws, regulations and
policies that produce racially prejudiced LTC outcomes. Medicaid’s
financial eligibility rules devastate the poor but enable higher income
individuals to qualify and preserve substantial exempt wealth. By
retaining “key money” to pay privately at market rates before converting
to Medicaid, the financially able access better facilities and services
than are available to enrollees unable to pay. By indemnifying the
nonneedy against LTC risk, Medicaid created a moral hazard that
discouraged LTC planning and left most people dependent on public
assistance when they face catastrophic care costs. The solution to
structural LTC racism is to eliminate Medicaid’s laws and regulations that
benefit the affluent and disfavor minorities.
Main Text: Long-term care (LTC),
also known as long-term services and supports, encompasses medical and
custodial care in residential or institutional settings for people in need
of assistance with activities of daily living due to frailty, disability
or cognitive impairment. Socially and economically marginalized groups
face impaired access to quality LTC in the United Sates. A rapidly
expanding academic literature documents disparities of many kinds.
Blacks tend to reside in nursing
homes that have “serious deficiencies, lower staffing ratios, and greater
financial vulnerability.”[1]
Besides dubious nursing homes, the range of deficiencies experienced
disproportionately by Black, Indigenous, and persons of color (BIPOC)
includes segregation;1,[2]
reduced access or deficient home and community-based care,[3],[4],[5]
assisted living,[6]
mental health services,[7]
pain medication,[8]
influenza vaccinations,[9]
hospital and hospice care[10]
and ADRD (Alzheimer’s Disease and Related Dementias) care;[11]
more physical restraints[12]
and pressure ulcers;[13]
and higher COVID-19 incidence, hospitalization and death counts.[14],[15]
Structural LTC Racism
What accounts for these inequities?
The common denominator is Medicaid dependency.[16]
Due to its dominance of LTC financing, contributing over half of the $438
billion the U.S. spent on LTC in 2022,[17]
and its low reimbursement rates, far below private-pay levels and often
less than the cost of providing the care,[18]
Medicaid is responsible for most of the deficient access and quality that
BIPOC patients receive. Because the long-term care system itself causes
racial disparities, many sources attribute the problems to “systemic,
structural or institutionalized racism.”[19],[20]
Structural racism “operates through laws and policies that allocate
resources in ways that disempower and devalue members of racial and ethnic
minority groups, resulting in inequitable access to high-quality care.”[21]
Residential segregation and poverty
cause BIPOC LTC users to live disproportionately in poor neighborhoods.
People with lower economic status who live in relatively impoverished
neighborhoods with nursing homes that rely most heavily on Medicaid’s
meager reimbursements tend to be the ones who suffer most from structural
LTC racism. Whites who depend on Medicaid are not immune to the same
deficiencies afflicting marginalized enrollee groups. But Whites on the
margin are more prosperous and less dependent on Medicaid. They tend to
live in areas with better private-pay LTC options, such as home care and
assisted living, and with nursing homes that are less Medicaid dependent.[22]
Proposed Solutions for Structural
LTC Racism
Proposals to eliminate or mitigate
structural LTC racism center on improving Medicaid with better policies
and more funding. One source calls for a multi-prong effort to add
“disproportionate-share payment adjustments to nursing homes with a higher
proportion of Medicaid residents” and to equalize “Medicaid and
private-pay payments.”1 Another would “increase Medicaid and
Medicare reimbursement rates, especially for providers serving high
proportions of Medicaid-eligible and BIPOC older adults” and “expand
access to Medicaid-waivered HCBS services.”20 These are worthy
goals, but simply pouring more resources into Medicaid without eliminating
the conditions that favor Whites over BIPOC patients would only deliver a
better funded, but still structurally racist program.
Absent from the large body of
peer-reviewed articles on structural LTC racism is much discussion of the
specific “laws, policies, institutional practices, and entrenched norms”
that disempower racial and ethnic minorities and cause the care
disparities.[23]
If Medicaid dependency triggers the LTC system’s inequities and
deficiencies, then the laws and policies governing Medicaid LTC
eligibility should be a crucial topic for analysis. What are those laws
and policies? What role do the rules governing access to Medicaid LTC
benefits play? Do they benefit some and disadvantage others? If so, how
are marginalized groups disempowered and devalued? Do prosperous people
benefit disproportionately from Medicaid? If so, how?
Medicaid and Structural LTC
Racism
Income and Asset Eligibility
Rules
The most common statement about
Medicaid LTC eligibility in both the popular and academic literature is
that qualification requires low income and assets. Sources explain that
income above $943 per month ($967 as of 2025) or assets exceeding $2,000
renders someone ineligible for the program. Applicants must “spend down”
privately for care to those levels before they become financially
eligible. In fact, however, Medicaid LTC financial eligibility is much
less stringent.
Income is rarely an obstacle to
eligibility because state Medicaid programs either deduct private health
and LTC expenses before applying the low income standard or they permit
applicants to divert excess income into trusts. Most states (34) use the
“medically needy” income eligibility method.[24]
They deduct private medical and LTC expenses from income before
determining eligibility, enabling people to qualify despite having incomes
well above categorical eligibility limits. Other states use an “income
cap” method, allowing income up to 300 percent of the Supplemental
Security Income monthly limit. People with much higher incomes can still
qualify for Medicaid in income cap states by diverting excess income to an
income diversion trust, also known as a “Miller” or “Qualified Income
Trust.”[25]
A rule of thumb is that income below the monthly cost of a nursing home,
easily $8,000 or $9,000, relatively high income, is not disqualifying.
Likewise, most large resources
seniors own are exempt from Medicaid’s asset limit. Exempt wealth includes
a home and all contiguous property up to a minimum of $713,000 ($730,000
as of 2025) everywhere and a maximum of $1,071,000 ($1,097,000 as of 2025)
or more in nine states,[26]
but also, without any dollar limit, one vehicle, prepaid burial funds, a
business including its capital and cash flow, personal belongings and
household furnishings, even IRAs if they are in payout status as is
usually true for elders in need of LTC.25
Medicaid Financial Eligibility
and Structural LTC Racism
How do these facts about Medicaid
LTC income and asset eligibility relate to structural LTC racism? Most low
income, asset-poor people qualify for Medicaid LTC benefits quickly. They
have little income and countable wealth to spend down and what they do
have is consumed rapidly by private health and LTC expenditures. Medicaid
LTC financial eligibility policy devastates people on the lowest rung of
the wealth ladder.
Less understood is that many people
with substantially greater wealth also qualify quickly and with little or
no asset spend down required. Their biggest assets, such as home equity,
are exempt already and their countable resources are easily converted to
exempt status. They can “spend down” countable assets simply by purchasing
a new car, home improvements or any other item on long lists of exempt
assets available online,25 or from attorneys specializing in
Medicaid planning.[27]
Medicaid planners routinely qualify
even wealthy clients for Medicaid LTC benefits by means of legal spend
down avoidance strategies such as Medicaid asset protection trusts used
“to protect assets from being counted for Medicaid eligibility;”[28]
Medicaid-compliant annuities that convert “excess funds into an income
stream with no cash value” to accelerate “Medicaid eligibility, while
protecting your client’s assets;”[29]
life estates “to preserve your residence and increase your Medicaid
eligibility,”[30]
or half-a-loaf methods. “Half a Loaf, Reverse Half a Loaf, and Modern Half
a Loaf are Medicaid gifting strategies (also called transfer strategies) …
used for the purpose of reducing countable assets to qualify for Medicaid.
These strategies can also preserve some of the Medicaid applicant’s assets
for their family members.”[31]
California’s Medi-Cal program recently eliminated its limit on countable
assets altogether making LTC benefits available regardless of wealth and
obviating the need for sophisticated legal spend down strategies.[32]
One effect of this system is that
middle-class and affluent people qualify for Medicaid LTC benefits as
easily as the poor and with less financial disruption. Once qualified, all
use Medicaid’s LTC benefits. When people of moderate or substantial wealth
qualify for Medicaid, they consume scarce resources that would otherwise
have benefited people of lesser means. Such expanded coverage depletes
Medicaid’s scarce resources and reduces the range and quality of care
available to others on the program, especially BIPOC enrollees.
But why would people who could
purchase high quality LTC in the private market prefer to qualify for
Medicaid instead? Is it only to save money? Or could they somehow capture
the best care Medicaid has to offer to the exclusion of more disadvantaged
enrollees? How biased is Medicaid-based structural LTC racism?
Key Money[33]
It seems counter-intuitive that
individuals and families with significant wealth would choose to use
Medicaid even when that path is legally available to them given the
program’s reputation for substandard access and quality. The reason they
do is one of the many ways structural LTC racism manifests in the LTC
marketplace.
Some nursing homes have relatively
few Medicaid beds. Such facilities often have supplemental philanthropic
funding and comparatively high private-pay or Medicare resident census.1
They enjoy the higher financial margins that come from those sources’
relatively more generous reimbursements. Such facilities often provide
better care and services because of their higher revenue and lesser
dependency on low Medicaid rates. This two-tier system benefits those who
can access it, but disadvantages any, including many BIPOC enrollees, who
cannot.16
Because the Medicaid reimbursement
rate for nursing home care is approximately 70 percent of what private
payers pay,[34]
skilled nursing facilities eagerly seek out new admissions who can pay
privately from day one and for at least some period of time before they
convert to Medicaid.1 Medicaid planners encourage their
affluent clients to hold back enough countable wealth, so-called “key
money,” from the Medicaid spend down process so they will be able to pay
privately for care at the start “to facilitate the admission of the
Medicaid applicant to the best long-term care facility available.”[35]
Once admitted, nursing homes cannot evict patients simply because their
source of payment changes from private pay to Medicaid.[36],[37]
Because socioeconomically
disadvantaged groups lack key money, they end up in the less desirable
Medicaid-only or mostly Medicaid facilities. More prosperous White
enrollees tend to live in areas with the best LTC facilities and they
possess the key money to buy their way in. This result is unfair,
unethical, and structurally racist, but commonplace.[38]
Moral Hazard
Beyond consuming Medicaid resources
that could have gone to economically marginalized people, the availability
of Medicaid LTC benefits to individuals of higher financial means has
another negative, systemic consequence. In effect since Medicaid began
operating in 1966, this system created a moral hazard—“a situation in
which people or organizations do not suffer from the results of their bad
decisions, so may increase the risks they take.”[39]
The result of making Medicaid LTC eligibility available late in life while
allowing significant wealth to be divested or retained in exempt form is
that too many people fail to plan for LTC.[40]
They end up consuming Medicaid resources instead. Why save, invest or
insure early in life against needing LTC someday in old age when the
government covers catastrophic costs if such care is needed and reserves
the best publicly financed care for the most economically well-off people?
This harmful incentive discourages early, responsible LTC planning by
relatively prosperous people. It underwrites structural LTC racism.
Roots of Structural LTC Racism
Medically Needy Eligibility
From the beginning, Medicaid LTC
benefits were available not only to the financially destitute, those
meeting the strict financial qualifications for state welfare payments or
Supplemental Security Income (SSI), but also to the medically needy. The
medically needy are people with too little income to pay for institutional
or home-based LTC, but with too much income to qualify for cash
assistance. These higher income people are not excluded from Medicaid
eligibility based on income if their private health and LTC expenses are
high enough or they use an income diversion trust. The result is that
people with significant incomes end up relying on Medicaid. The same
people preserve wealth in the form of exempt assets. While such assets are
vulnerable to mandatory estate recovery, few states enforce that
requirement effectively and the liability is easy to avoid with some early
legal planning.[41]
Law makers’ well-intentioned plan to
help more people with LTC disinclined everyone to prepare personally for
LTC risk and overloaded the public assistance program with enrollees.
Medicaid LTC tried to do too much for too many so it does too little for
most, especially for BIPOC enrollees with the greatest need. That is the
root of structural LTC racism.
LTC Financing and Racism
Medicaid LTC enrollees are required
to contribute most of their income to offset the program’s cost for their
care. As Medicaid reimbursement rates are only about two-thirds of
private-pay rates, enrollees get a substantial discount on their care.34
But LTC providers are short-changed. They receive only the Medicaid rate,
often less than the cost of the care, instead of the higher private-pay
rate even though enrollees are paying “out-of-pocket” from their incomes,
largely from their Social Security benefits. It sometimes happens that
enrollees’ incomes are higher than Medicaid’s rate for their care. In
those cases, Medicaid pays nothing; the enrollee pays all; and the LTC
provider struggles financially with most of its revenue coming from the
lowest payors’ rate. As the structural LTC racism literature often
observes, low Medicaid reimbursements cause care deficiencies and
inequities. These occur because of the laws and policies that govern
Medicaid LTC eligibility and financing.
A Solution for Structural LTC
Racism
If the cause of structural LTC
racism is too many enrollees with sheltered or divested wealth
overwhelming Medicaid’s ability to pay for quality care, then the solution
must lie in diverting more prosperous people away from Medicaid
dependency, enabling them to pay privately for LTC, and thus empowering
Medicaid to afford better care for those most in need who remain eligible.
But that is a tall order. It presents two major challenges: (1) how to
keep people with significant wealth off Medicaid so more program resources
reach the people currently shortchanged by structural LTC racism, and (2)
how to prepare the middle class and affluent to pay for their own LTC when
they need it after Medicaid is no longer available to pay for their care
and preserve their wealth as now.
Re-targeting Medicaid to end
structural LTC racism
Knowing how to exclude
higher-income/higher-asset people from Medicaid LTC so that more program
resources reach the disadvantaged is not difficult. Simply repeal the
Medicaid laws, regulations and policies that permit them to qualify.
Medically needy income eligibility rules that allow higher income people
to qualify if their private health and LTC expenses are high enough should
end. Practically unlimited asset exemptions, such as for home equity, that
permit people with any amount of wealth to qualify must go. Spending down
by purchasing exempt assets instead of paying for care should cease.
Medicaid strategies such as special trusts, annuities, spousal refusal,
and life estates—legal gimmicks that enrich lawyers and their affluent
client heirs—must stop as well. Easing the path to Medicaid’s best LTC
options by means of key money should end. Stopping structural LTC racism
cannot be achieved until Medicaid is preserved exclusively for the most
disadvantaged, whom its laws and policies have hurt the most historically.
But these needed changes are much
more difficult to achieve politically than they are to identify and list.
People who benefit from the status quo will fight to preserve and expand
the current system and structure. These interested parties include (1)
most Americans who remain oblivious to LTC risk and cost because easy
access to Medicaid LTC late in life has enabled their denial; (2) elder
law attorneys and financial planners who profit from transitioning
prosperous clients to the best of Medicaid-financed care; (3) politicians
who garner votes by promoting easy access to Medicaid LTC benefits; (4)
LTC analysts and economists who ignore the extensive legal literature on
Medicaid planning and pretend the practice of artificial impoverishment
does not occur, and (5) the state and federal health and human services
bureaucracies that have strived to expand Medicaid LTC to everyone,
especially the White middle class, instead of targeting it to the victims
of structural LTC racism. These are the people and the reasons that
sustain the LTC status quo and stand in the way of reform, consistently
protecting structural LTC racism whether consciously and intentionally or
not.
Conclusion
Structural LTC racism causes reduced
access to quality LTC for marginalized groups. It is grounded in Medicaid
LTC eligibility law, regulations and policies. By enabling middle class
and affluent people to access Medicaid LTC late in life, and preserve
exempt wealth, the program became overloaded with people who should, could
and would otherwise have prepared privately for LTC risk and cost.
Medicaid covered too many enrollees with too many benefits ensuring that
those most vulnerable financially would receive the program’s deficient
care, while others more privileged, in possession of key money, would gain
access to the best care the program offers.
The good news is that this condition
is reversible. Lawmakers should end access to wealth-preserving Medicaid
LTC benefits late in life. Instead, offer creative methods for families in
mid-life to prepare responsibly to pay privately when and if they ever
need expensive extended care. Some possibilities include allowing
individuals and families to meet individually set LTC saving goals by
carving out portions of other wealth they are accumulating, such as from
retirement savings, home equity, life insurance or estate planning.
Implement such measures and enormous, desperately needed private funds
will flow immediately into the LTC service delivery system ensuring better
access to higher quality care for everyone. Relieved of financing LTC for
the middle class and affluent, Medicaid will be able to pay adequately to
ensure quality care for all enrollees, ending the long-standing system of
structural LTC racism.
Why this goal is realistic and how
to achieve it are topics for another paper.
[1]
Smith DB, Feng Z, Fennel ML, Zinn JS, Mor V. Separate and unequal:
racial segregation and disparities in quality across U.S. nursing
homes. Health Aff 2007;26:1448—1459.
[2]
Rahman M, Foster AD. Racial segregation and quality of care disparity
in US nursing homes. J Health Econ 2015;39:1—16.
[3]
Fabius CD, Ogarek J, Shireman TI. Racial disparities in Medicaid home
and community-based service utilization among White, Black, and
Hispanic adults with multiple sclerosis: implications of state policy.
J Racial Ethn Health Disparities 2019;6:1200—1207.
[4]
Zhanlian F, Fennell ML, Tyler DA, Clark M, Mor V. Growth of racial and
ethnic minorities in US nursing homes driven by demographics and
possible disparities in options. Health Aff 2011;30:1358—1365.
[5]
Gorges RJ, Sanghavi P, Konetzka RT. A national examination of
long-term care setting, outcomes, and disparities among elderly dual
eligibles. Health Aff 2019;38:1110—1118.
[6]
Morales MJ, Robert SA. Black–White Disparities in Moves to Assisted
Living and Nursing Homes Among Older Medicare Beneficiaries. J
Gerontol Soc Work 2020;75:1972—1982.
[7]
Rivera-Hernandez M, Kumar A, Epstein-Lubow G, Thomas KS. Disparities
in nursing home use and quality among African American, Hispanic, and
White Medicare residents with Alzheimer’s disease and related
dementias. JAH 2019;31:1259—1277.
[8]
Mack DS, Hunnicutt JN, Jesdale BM, Lapane KL. Non-Hispanic Black-White
disparities in pain and pain management among newly admitted nursing
home residents with cancer. J. Pain Res. 2018;11:753-761.
[9]
Travers JL, Schroeder KL, Blaylock TE, Stone PW. Racial/ethnic
disparities in influenza and pneumococcal vaccinations among nursing
home residents: a systematic review. Gerontologist 2018;58:205—217.
[10]
Zheng NT, Mukamel DB, Caprio T, Cai S, Temkin-Greener H. Racial
disparities in in-hospital death and hospice use among nursing home
residents at the end-of-life. Med Care 2011;49:992-998.
[11]
Rivera-Hernandez M, Kumar A, Epstein-Lubow G, Tomas KS. Disparities in
nursing home use and quality among African American, Hispanic, and
White Medicare residents with Alzheimer’s Disease and Related
Dementias. J Aging Health 2019;31:1259—1277.
[12]
Cassie KM, Cassie W. Racial disparities in the use of physical
restraints in U.S. nursing homes. Health Soc Work 2013;38:207—213.
[13]
Cai S, Mukamel DB, Temkin-Greener H. Pressure ulcer prevalence among
Black and White nursing home residents in New York state: evidence of
racial disparity? Med Care 2010;48:233—239.
[14]
Gorges RJ, Konetzka RT. Factors associated with racial differences in
deaths among nursing home residents with COVID-19 infection in the US.
JAMA Netw Open 2021;4:e2037431.
[15]
Khazanchi R, Evans CT, Marcelin JR. Racism, not race, drives inequity
across the covid-19 continuum. JAMA Netw Open 2020;3:1—3.
[16]
Mor V, Zinn J, Angelelli J, Teno JM, Miller SC. Driven to tiers:
socioeconomic and racial disparities in the quality of nursing home
care. Milbank Q 2004;82:227—256.
[18]
Gruneir A, Miller SC, Feng Z, Intrator O, Mor V. Relationship between
state Medicaid policies, nursing home racial composition, and the risk
of hospitalization for Black and White residents. Health Serv Res
2008;43:869—881.
[19]
Jones CP. Levels of racism: a theoretic framework and a gardener’s
tale. Am J Public Health 2000;90:1212—1215.
[20]
Shippee TP, Fabius CD, Fashaw-Walters S, Bowblis JR, Nkimbeng M, Bucy
TI, et al. Evidence for action: addressing systemic racism across
long-term services and supports. J Am Med Dir Assoc 2022;23:214—219.
[21]
Yearby, R, Clark B, Figueroa JF. Structural racism in
historical and modern US health care policy. Health Aff
2022;41—187-194.
[22]
Sloane PD, Yearby R, Konetzka RT, Li Y, Espinoza R, Zimmerman S.
Addressing systemic racism in nursing homes: a time for action. J Am
Med Dir Assoc 2021;22:886—892.
[23]
Braveman PA, Arkin E, Proctor D, et al. Systemic and structural
racism: definitions, examples, health
damages, and approaches to dismantling. Health aff
2022;41:171—178.
[24]
Musumeci MB, Chidambaram P, Watts MO. Medicaid financial eligibility
for seniors and people with disabilities: findings from a 50-state
survey. KFF 2019
LINK. Accessed July 13, 2024.
[25]
American Council on Aging. Spending down assets to become Medicaid
eligible for nursing home/long term care.
LINK. Accessed July 13, 2024.
[26]
American Council on Aging. Impact of home ownership on Medicaid
eligibility considering marital status & Medicaid type.
LINK. Accessed July 13, 2024.
[27]
American Council on Aging. Medicaid planning: definition, costs &
types of planners,
LINK. Accessed July 13, 2024.
[28]
Law Offices of Stephen J. Silverberg. What is a Medicaid asset
protection trust (MAPT).
LINK. Accessed July 13, 2024.
[29]
Krause Financial Services. Medicaid compliant annuity.
LINK. Accessed July 13, 2024.
[30]
The Retirement Group. Residence Transfer Subject to Life Estate:
Medicaid Planning for Merck Employees and Retirees.
LINK. Accessed July 13, 2024.
[31]
American Council on Aging. How the modern half a loaf strategy helps
families become Medicaid eligible and preserves assets.
LINK.
Accessed July 13, 2024.
[32]
California Health Advocates. Medi-Cal’s asset limit is now eliminated.
LINK. Accessed July 13, 2024.
[33]
Kenton W. Key money: what it is, how it works, in practice.
LINK. Accessed July 13, 2024.
[34]
American Council on Aging. 2021 nursing home costs by state and
region, understanding the difference between private pay and medicaid
reimbursement.
LINK.
Accessed July 13, 2024.
[36]
Elder Law Answers. Fighting nursing home discrimination against
Medicaid enrollees.
LINK. Accessed July 13, 2024.
[37]
California Advocates for Nursing Home Reform. Overview of Medi-Cal for
long term care.
LINK. Accessed July 13, 2024.
[38]
Warshawsky MJ. Steps to make long-term care financing fairer and more
sustainable. Tax Notes Federal 2022;176:973—988.
[39]
Cambridge Dictionary.
LINK. Accessed July 13, 2024.
[40]
Brown JR, Finkelstein A. Insuring Long-Term Care in the United States.
JEP; 2011: 119-142.
[41]
Super Lawyers. Avoiding pay back: Medicaid planning and estate
recovery: protecting your assets from state reimbursement for nursing
home care costs.
LINK. Accessed July 13, 2024.
#############################
Updated Monday, May 12, 2025, 10:03
AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-017:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Suozzi Looks To Trim Costs Of His Public Long-Term
Care Insurance Plan
-
Employees with higher incomes, education levels
more likely to anticipate need for long-term care
-
Skilled nursing workers more prone to violence,
injuries than any other healthcare sector: study
-
Elder Law Planning: Safeguarding Your Assets And
Securing The Best Care
-
2 in 7 say low pay will be the reason they leave
senior care sector: study
-
The age-old problem of long-term care
-
More than 1 in 5 Medicare home health users have
unreported dementia, study finds
-
Americans with Alzheimer’s tops 7 million, new
report shows
-
Fate Worse Than Death: Many Long-Term Care
Residents Lose All Independence, Study Says
-
VA Nursing Home Care: Opportunities Remain to
Enhance Oversight of State Veterans Homes
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Monday, May 2, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC
Bullet: Five Things You Probably Don’t Know about Long-Term Care
LTC Comment:
What if most of what we think we know about long-term care is wrong? Let’s
explore some possibilities after the ***news.***
*** WEDNESDAY,
I participated in an “Alliance
for Health Policy” event in Washington, DC. The Alliance’s annual
Signature Series addresses challenging issues in health policy “by
convening cross-sector dialogue with experts in both policy and practice”
to “critically examine and identify what’s at stake, as well as key areas
of opportunity.” Last year’s theme focused on the transformative power of
Artificial Intelligence (AI) in health care and health policy. This year’s
theme is “aging.” Participants imagined what it would be like to be 80
years old (easy for me) and considered what challenges being that age
could bring to various demographic scenarios.
I’ll be back
in DC next week for Genworth and CareScout’s Symposium on “Sustainable
Solutions: The Future of Long-Term Care Financing.” Check out the
program’s landing page
here, where you can read about each of the four panels and review the
panelists’ bios. Join us virtually for the Symposium
here. I’ll be on Panel #4: "Better Together..." – Public + Private
Collaboration. Expect some spirited discussion. ***
LTC BULLET:
FIVE THINGS YOU PROBABLY DON’T KNOW ABOUT LONG-TERM CARE
LTC Comment:
Will Rogers is famously quoted as saying, "It isn't what we don't know
that gives us trouble, it's what we know that ain't so." No truer words
have been spoken about long-term care. Here are some thoughts and
considerations on that theme. I may develop these notes into a paper, but
for now just see what you think and feel free to offer feedback to
smoses@centerltc.com.
“Five Things
You Probably Don’t Know about Long-Term Care”
by
Stephen A.
Moses
-
Very little
private wealth funds LTC
a. $97 trillion wealth in …
i. Retirement savings ($40T),
ii. Home
equity ($35T)
iii. Life
insurance ($22T)
b. LTC
spending: $629.3B
i. Medicaid:
$278.3B, 44.2%
ii. Medicare:
$100.3B, 15.9%
iii. Private
insurance and other public payers: $169.0, 26.9%
iv. Out
of pocket: $81.7B, 12.9%
1. Half
is income of people already on Medicaid
a. Mostly
Social Security income
b. But
pension and other private income too
2. Only
half could be spend down of savings
a. $40.9B,
6.5%
b. $1
out of $15 spent on LTC
-
Medicaid is good for the affluent,
bad for the poor
a. Medicaid
treats the affluent well
i. High
income people qualify (medically needy)
ii. High
asset people qualify (exempt wealth)
iii. Affluent
people get the best Medicaid offers
1. Key
money
iv.
Medicaid is a windfall
for affluent heirs
1. Big
exemptions
2. Little
estate recovery
b. Medicaid
treats the poor poorly
i. Few
assets wiped out quickly
ii. Lack
key money, so …
1. Shunted
to the worst, high-Medicaid nursing homes and home care providers
iii. Victims
of “LTC
racism”
-
Medicaid no longer prioritizes the
poor aged, disabled and dual eligibles (“How
the Wealthy Stole Medicaid”)
a. Since
ACA, Obama Care, in 2010
i. 90%
federal match; $9 federal for every $1 state
ii. Covers
working age adults with incomes up to 138 percent of the federal poverty
level
iii.
Mostly single, often unemployed, childless people incentivized to remain
so and to attract others to the same generous benefit
b. Expansion
population grew from nothing to 20% of Medicaid dollars
c. Aged
and disabled
i. Went
from 25% of enrollees and 69% of expenditures (2003)
ii. To
20% and 50%, respectively (2023)
d. Dual
eligibles
i. From
14% and 42% (2005) to 14% and 32% (2023)
-
LTC financing is schizophrenic
a. Diametrically
contradictory public policies
i.
Reward accumulation of
wealth, such as
tax-favored IRAs and 401(k)s that build nest eggs;
subsidized mortgages and
mortgage-interest tax deductions that grow home equity; and
tax-deferred growth and tax-free death benefits that boost life
insurance cash value.
ii. Medicaid
eligibility policies that discourage spending for LTC
1. Punish
the poor
2. Reward
the affluent.
b. Results
i. Plenty
of private funds in the economy lie fallow for LTC financing
1. Less
full price revenue for LTC providers
2. LTC
access and quality suffer
ii. As
those funds are not at risk, LTC insurance market to protect them lags
1. People
ignore LTC until they need it
2. Then
qualifying for Medicaid is the path of least resistance
iii. Too
many people rely on Medicaid, with dire consequences
1. Poor
reimbursements
a. Caregiver
shortages
b. Deficient
care
c. Too
little HCBS
d. Nursing
home closures
2. Institutional
bias
a. Decades
warehousing elderly in nursing homes
b. Still
problem in rural areas
3. Discrimination
a. In
favor of private payers
i. Key
money
ii. Access
to best institutional and home-based care
b. Against
Medicaid recipients
i. LTC
racism
ii. Condemned
to high-Medicaid, poor quality care
4. Moral
hazard
a. Easy
access to Medicaid caused …
b. Complacency,
resulting in …
c. Failure
to plan, save, invest or insure in LTC
-
A public/private LTC solution does
not require a big, new, compulsory, payroll-funded entitlement and trust
fund
a. Medicaid
must pay market rates
i. Eliminate
discrimination against poor and for affluent
ii. LTC
providers pay adequate wages
1. Solves
caregiver shortage
2. Ensures
caregiver quality
iii. Competition
1. For
private payers
2. Instead
of begging for more Medicaid
iv. But
Medicaid cannot pay market rates with so many on the program
1. Must
reduce Medicaid census
2. Increase
private financing
a. Put
$97 trillion private wealth to work
b. Attract
LTC insurance to protect the wealth
b. Solutions
to reduce Medicaid dependency and attract private wealth to LTC
i. Keep
Medicaid treatment of income the same
1. Continue
to require income spend down for care (medical or LTC)
2. Excess
Social Security, pension and other private income offsets Medicaid costs
3. But
LTC providers receive market rates, not Medicaid’ previous below-cost
rates
ii. Stop
allowing spend down by purchasing exempt assets (“Medicaid's
$100+ Billion Leak”)
1. Asset
spend down does not have to be for care costs currently
a. Unlike
income spend down
b. Allows
conversion of unlimited countable wealth to exempt status
2. So
make them the same
a. Potential
savings of $100+ billion per “class” of elders
i. New
“class” of infirm elders every two or three years
iii. Eliminate
or radically reduce Medicaid’s huge home equity exemption
1. Let
seniors’ $14 trillion of home equity flow into LTC financing
2. Vast
new revenue potential for LTC providers
3. Better
access and quality
4. Strong
incentive to insure home equity early against LTC cost
iv. End
abusive Medicaid planning methods that benefit only the affluent
1. Irrevocable
trusts
2. Medicaid
compliant annuities
v. Extend
Medicaid’s five-year lookback to 10 years or 20
1. Easy
to check through assessors and recorders
2. Discourages
early planning for Medicaid LTC
vi. End
systemic LTC racism
1. When
all funders, including Medicaid, pay market rates …
2. Discrimination
based on payment source will end, and
3.
LTC racism will disappear.
vii. End
Obama Care preference for able-bodied, working-age adults
1. Stop
90% match for “expansion” population
2. Give
Medicaid back to the vulnerable poor, aged and disabled people it was
intended to serve
viii. Let
states experiment
1. Block
grants
a. Accept
less federal money
b.
Receive more policy flexibility
2. Experiment
with creative ways to do more with less
a. States
as laboratories of federalism
#############################
Updated Monday, April 28, 2025, 10:03
AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-016:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Baby Boomers Are No Longer Concerned About Their
Kids Future-Here’s Why
-
The Care Dividend Why and How Countries Should
Invest in Long-Term Care
-
Personal savings goals out of reach for most
Americans: survey
-
Why should societies invest in long-term care? New
evidence makes the case for action
-
In policy shift, Medicare makes family caregivers
part of medical reimbursement system
-
Medicaid Reform Goals + Paragon’s Latest on
Reducing Medicaid and Exchange Waste
-
Long-Term Care: Affording it Without Losing the
Farm
-
Long-term care insurance crisis: Soaring premiums,
policy buyouts, and ‘deceptive’ tactics
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Monday, April 21, 2025, 10:03
AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-015:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Americans plan to save less for retirement,
even though it won’t be enough, survey finds
-
An untapped resource: How family caregivers
provide value for home care
-
History Repeats? Faced With Medicaid Cuts,
States Reduced Support For Older Adults And Disabled People
-
Without support, seniors aging in place may
elect facility-based care, study finds
-
Medicare Advantage And Supplemental
Long-Term Services And Supports: A Small Step In The Right Direction
-
Hospital visits for cannabis use linked to
higher dementia risk
-
Unpacking dysfunction in long-term care
insurance
-
How cutting Medicaid would affect long-term
care and family caregivers
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Monday, April 18, 2025, 10:03
AM (Pacific)
Seattle—
#############################
LTC BULLET:
HOW THE WEALTHY STOLE MEDICAID
LTC Comment: Private
wealth sits on the sidelines as Medicaid shifts from helping the poor and
vulnerable to subsidizing the middle class and affluent. Facts and
analysis follow the ***news.***
|
*** TODAY'S LTC BULLET is sponsored by Claude
Thau (BackNine Insurance). BackNine gives you a free
personalized website at no cost. Your clients (& family & friends)
can, with as little or as much of your involvement as you or they
want, buy life insurance and LTCi, and can speed issue by scheduling a
paramed and uploading medical records immediately. We quote
stand-alone LTCi, linked-benefit and life with a LTC rider
side-by-side. Claude is the lead author of Milliman’s annual Broker
World LTCi Survey & a past Chair of the Center for Long-Term Care
Financing. Contact him at 913-707-8863 or
claude@back9ins.com to learn about more
great BackNine features and services. *** |
*** MCKNIGHTS LTC NEWS
COLUMNS by Steve Moses. From time to time, we point LTC Bullets
readers to columns I’ve published in
McKnights LTC News. McKnights is the leading publisher of news
about the LTC provider industry with separate publications focused on
nursing homes, senior living and home care. I think it is very important
for people working in the LTC financing side of the business to understand
the challenges people working in the provider side of the business face
and vice versa. These columns published in the past year are my way to
reach out and encourage mutual understanding between our professional
silos. I invite your feedback to
smoses@centerltc.com. If you find value in this work, remember it is
part of what you support when you join the Center for Long-Term Care
Reform. Please do that
here. Check out all our membership levels and benefits
here. Let’s fix long-term care together.
Are We LTC Suckers, April 11, 2025
Disrupt LTC Now, February 26, 2025
Where Did the Private Payers Go?, January 17, 2025
What’s Next for Long-Term Care?,
December 2, 2024
Long-term care policies matter, October 28, 2024
What if Medicaid Paid Market Rates?, September 16, 2024
How Medicaid cripples SNFs, August 12, 2024
What Assisted Living Needs Versus What It Gets, July 8, 2024
The Medicaid LTC snafu, April 15, 2024 ***
LTC BULLET: HOW THE
WEALTHY STOLE MEDICAID
Last week, the
Paragon Health Institute published “Medi-Cal-amity:
California’s Reckless Expansion of Medicaid Long-Term Care to the Affluent.”
In that policy brief, I explained how Medi-Cal eliminated its asset
eligibility test making even the richest Californians eligible for the
Medicaid program’s most expensive long-term care (LTC) benefits.
Unfortunately, that egregious misuse of the public welfare program in the
Golden State is only the tip of the iceberg nationally.
Medicaid has
transitioned for decades from a means-tested program intended to help the
poor and vulnerable into an entitlement for the middle class and affluent.
For example, the aged and disabled were 25
percent of enrollees in 2003, when they consumed 69 percent of total
Medicaid expenditures. By 2023, they had declined to
20 percent of enrollees receiving only 51 percent of total spending.
The poorest of the poor, “dual eligibles” who qualify for both Medicaid
and Medicare, were
14 percent of Medicaid enrollees in 2005 and accounted for 42 percent
of total program expenditures. By 2023 they remained 14
percent of enrollees but they garnered only 32 percent of spending.
Why are Medicaid’s most vulnerable recipients getting such short shrift
lately?
The 2010 Affordable Care
Act, aka Obama Care, created a new category of Medicaid recipients:
working age adults with incomes up to 138 percent of the federal poverty
level. State Medicaid programs receive a 90 percent federal funds matching
rate for services provided to this new group of enrollees. Compared to the
average match rate for other Medicaid eligibility groups of 50 to 77
percent depending on the state, this special, extremely high level makes
this “expansion” population very attractive. States need to put up only
$10 to receive $90 from the federal government. Responding to this
incentive, states have added
21 million recipients to Medicaid
enrollment nationally. These new, young, able-bodied recipients now
consume
20 percent of total Medicaid expenditures, 18 percent from federal
funds and two percent from states.
It is easy to see,
therefore, why the resources Medicaid formerly reserved for the poor
elderly and disabled are going instead to mostly single, often unemployed
people incentivized thereby to remain so and to attract others to the same
generous benefit. But there is another, possibly even more important way,
that Medicaid’s neediest and most vulnerable recipients are being crowded
out from access to the best care.
Over the years, by a
kind of eligibility bracket creep, more and more well-to-do people have
gained access to Medicaid LTC benefits without the inconvenience of
spending down their savings to pay privately for nursing home or home
care first. High income people qualify because Medicaid deducts their
private health care expenditures from their income before applying an
income test. Most elderly people in need of LTC have high private health
costs so they qualify easily based on income. For example, if a private
nursing home costs $10,000 per month, a Medicaid applicant with that much
income would qualify for Medicaid, transferring the cost of the nursing
home and other medical expenses to the program. While the patient’s income
would still go to the nursing home to offset Medicaid’s cost for the care,
the facility would receive only Medicaid’s below-cost reimbursement rate
instead of the much higher private pay rate. The Medicaid rate, at about
two-thirds of the private pay rate, severely inhibits the facility’s
ability to provide quality care for LTC patients on the program.
Likewise, people with
high assets routinely qualify for Medicaid LTC benefits, even when
countable assets are officially limited to $2,000 as in most states,
because nearly all of the elderly’s large assets are exempt from any spend
down requirement. Such exempt resources include most home equity, up to
$1,097,000 in some states but never less than $730,000 in any state except
California, which eliminated the asset test altogether making the home
equity limit moot. Also exempt, in unlimited amounts, are one business,
tax-favored retirement savings, a vehicle, prepaid burial funds, personal
belongings and home furnishings. As few states enforce mandatory estate
recovery, most of these exempt resources pass unencumbered to heirs who
reap a windfall from funds Medicaid protected from their parents having to
pay privately for their own LTC.
The two trends in
Medicaid policy just described—new able-bodied, working-age adults
capturing one-fifth of the program’s spending in the past 15 years while
high income and high asset people increasingly qualify easily for LTC
without first spending down their wealth—are converting Medicaid from a
safety net for the needy into an entitlement for the indolent and
affluent. There should be little wonder why few people take the risk and
cost of future LTC seriously enough to save, invest or insure in
preparation. Nor should we be surprised that so little private spending
goes to pay for LTC as this table of National Health Expenditure data
shows:
Only 12.9 percent of
total LTC spending comes “out of pocket.” But even that low amount is
deceiving as it includes income people on Medicaid must contribute to
offset the program’s cost for their care. Removing that income, mostly
from Social Security benefits, we find that only about 6.5 percent of
total LTC spending, $1 out of $15, could come from asset spend down. No
wonder people don’t worry about LTC until they need it and gravitate
quickly to Medicaid when costs of care escalate.
For these reasons,
America’s LTC financing system is rapidly spiraling into an inadequately
funded, welfare-based, centrally planned, government-run failure that
serves no one well, and especially not the neediest aged and disabled
recipients it is supposed to have served primarily. How can we reverse
this process of collapse? Step one is to remove the ACA expansion group
from Medicaid eligibility or, short of that, to radically reduce their
federal matching rate so that states have no special incentive to add
them compared to supporting traditional coverage groups such as poor
women, children, the aged and disabled. Step two is to divert the middle
class and affluent toward early planning for LTC and away from eventual
dependency on Medicaid. Achieving that objective requires tightening
Medicaid LTC financial eligibility rules, enforcing mandatory estate
recovery, and prohibiting the use of special trusts and annuities to
qualify while sheltering large sums of wealth. For details on how to do
that, see the
Paragon Health Institute’s “Long-Term
Care: The Problem,” “Long-Term
Care: The Solution,” and
Medicaid's $100+ Billion Leak.
If we give Medicaid back
to truly needy poor women and children, the aged and disabled, what can we
expect to happen? Medicaid census will plummet. Covering many fewer
genuinely eligible recipients, the program will be able to pay market
rates for services across the LTC spectrum: home care, assisted living and
nursing home care. That will end the discrimination against Medicaid
recipients that occurs because LTC providers are desperate to attract
private payers at 1.5 times the rate Medicaid pays. It will end the “LTC
racism” that occurs when the needy are crowded out from the best
nursing home and home care services because they lack “key money” to pay
privately for a while which opens doors to the best care for the affluent.
But where will the money
come from to pay private rates to LTC providers across the care spectrum?
Money in the U.S. economy for this purpose is not in short supply. It is
simply diverted from funding LTC by Medicaid financial eligibility
policies that discourage its use. In fact, Americans own $97 trillion in
retirement savings ($40T),
home equity ($35T),
and life insurance ($22T)
that could go to pay for their LTC when needed if it were not diverted
from that purpose by generous Medicaid income and asset eligibility rules.
More importantly, if and when that wealth becomes liable for LTC funding
due to changing Medicaid rules as recommended above, the public will act
early and responsibly to protect it against LTC risk and cost thereby
unleashing a long dormant market for private LTC insurance.
All that is needed is to
resolve the glaring contradiction in public policies that on the one hand
reward accumulation of wealth, such as
tax-favored IRAs and 401(k)s that build nest eggs,
subsidized mortgages and
mortgage-interest tax deductions that grow home equity, and
tax-deferred growth and tax-free death benefits that boost life
insurance cash value, and on the other hand divert those private assets
from LTC spending by making Medicaid financial eligibility so easy to
achieve while preserving wealth. The secret to fixing LTC is to keep those
public policies that grow wealth, but to repeal the policies that divert
that wealth from paying privately for LTC. Doing that will flood the LTC
service delivery system with desperately needed market-rate revenue and
unleash the suppressed potential of private LTC insurance. Everyone will
be better off including the genuinely needy who will receive better care
from Medicaid and most Americans who will access better care as private
payers.
Changes of this nature
and magnitude are a big ask, but they are based on evidence and sound
reasoning. Nothing ventured, nothing gained.
#############################
Updated Monday, April 14, 2025, 10:03
AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-014:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Administration’s deregulation push gives skilled
nursing providers an extra chance to shape the rules
-
Are We LTC Suckers
-
LTCi becoming more of a target for fraud
-
Medicare Advantage Payments to Increase Again
-
Getting Serious About Medicaid Reform + Several
Biden Health Policies Fall
-
A fifth of Americans are on Medicaid. Some of them
have no idea.
-
BREAKING: Judge tosses nursing home staffing rule
-
Study shows need for paid caregivers: 86 percent of
people living with dementia lack formal support
-
Medicaid Eligibility Levels for Older Adults and
People with Disabilities (Non-MAGI) in 2025
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Monday, April 7, 2025, 10:03
AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-013:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Senior living giant Pacifica files for Chapter 7
bankruptcy
-
Home care aides largest occupation in US as of last
May, BLS reports
-
Retirement becoming ‘moving target’ as older adults
wrestle with debt
-
CareScout Partners with Dr. Judy Benjamin on Her
Walk Across America
-
Family Caregivers Need Help. These Are the Policies
They Say Would Make the Biggest Difference
-
Is it time for the federal government to become
more involved in assisted living?
-
Long-Term Care Planning: What Gen X Needs To Know
Now
-
Memory Lane Games
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Monday, April 4, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC
BULLET: CARESCOUTING LTC
LTC Comment: This year’s Genworth/CareScout
cost of care survey is a marvelous tool. Details after the ***news.***
*** MORE CARESCOUT NEWS:
4/3/2025,
“CareScout
Partners with Dr. Judy Benjamin on Her Walk Across America,”
Genworth/CareScout
Quote:
“On Saturday, April 5, Judy Benjamin, PhD, a National Board-Certified
Health and Wellness Coach, will take her first steps on the more than
3,000-mile journey across the country to raise awareness for alternative
ways to stay healthy at any age. Over five months, she will walk from San
Diego, California, to St. Augustine, Florida, following the Adventure
Cycling Association Southern Tier route. … CareScout, a leader in
long-term care and aging solutions, is proud to partner with and support
Dr. Benjamin on this journey. This collaboration reflects and reinforces
CareScout’s commitment to empowering individuals and families with the
knowledge and resources to plan for aging with confidence and dignity.”
LTC Comment:
Go Judy! Go CareScout! ***
LTC BULLET: CARESCOUTING LTC
LTC Comment: The Boy Scouts’ motto is
“Be Prepared.” When it comes to long-term care (LTC) planning, there is
one tool all consumers should study carefully to become prepared.
Genworth and CareScout (Center-corporate-members) released their
2024 Cost of Care Survey results on March 4, 2025. This is the
survey’s 20th annual iteration and it has evolved to be a highly valuable
interactive tool.
As always, CareScout gives us the
latest account of care costs by type showing the traditional categories as
below. (I’m intentionally not focusing here on the data. Go to the source
for that. For now, just consider how vast and valuable the extractable
information is.)
In-home care
Homemaker
services
Home health
aide
Community and assisted living
Adult day
health care
Assisted
living community
Nursing home care
Semi-private
room
Private room
How do you want to see the cost of
care displayed? Hourly? Daily? Monthly? Annually? One click displays the
relevant data however you want to read it.
Want to check costs in your state of
residence? Simple. Just click your state on the U.S. map. Then, again,
choose hourly, daily, etc.
Maybe your big concern is the trend in
care cost. Scroll down to find a table showing 2024 and 2023 national
median values for hourly home care, daily adult day health, and monthly
assisted living and nursing home costs followed by their annual percent
change (increase). None of these categories went down in cost. Some went
up dramatically, such as hourly homemaker services (10 percent), monthly
assisted living (10 percent) and monthly nursing home for a semi-private
room (the level that Medicaid funds) (7 percent).
Keep scrolling down to find charts
showing the increase in all the categories over the past two years. If
that doesn’t scare you enough, try this …
Go back almost to the top of the
website and look for “Calculate Future Cost.” Now pick any decade from
2024 to 2074 and click for the estimates of future costs from CareScout’s
crystal ball. Want to fine tune even more? You can pick any year in
between. On top of that, you can still choose whether to see hourly,
daily, monthly or annual data!
But wait, there’s more! (I feel like a
pitchman.) CareScout lets you choose your expected rate of inflation from
one to five percent. Given that some care categories are rising in cost
faster than five percent already, 1 to 5 percent, may be too conservative,
so that should be taken into account.
By now, CareScout surely has your
attention. But maybe it’s too late for these numbers to scare you straight
into searching for a LTC insurance policy. In that case, CareScout offers
a link to “Find
Quality Care.” There you’ll find “726 CareScout Quality Network
Providers.”
Your
Center for
Long-Term Care Reform has posted links to the annual Genworth/CareScout
cost-of-care surveys on our members-only website (The Zone) every year
since 2004. Click
here to join the Center and get your own user name and password.
You’ll find tons of useful information in The Zone and you’ll receive our
weekly LTC E-Alerts and bi-weekly LTC Bullets. Want daily
insights about everything happening in LTC? Become a premium member to
receive our daily LTC Clippings. Find all our individual and
corporate “Membership Levels and Benefits”
here.
#############################
Updated Tuesday, April 1, 2025, 10:03
AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-012:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Nursing homes fear states will be unable to fill
Medicaid 'hole' without provider taxes
-
Major job cuts, restructuring at HHS raises many
questions, industry group says
-
Can you use home equity to pay for long-term care?
-
A closer look at who relies on Medicaid
-
New Report: Addressing Medicaid Money Laundering
-
Aging farmers face long-term care challenges: OSU
Extension offers planning tools
-
Another shot at redemption?
-
Red States Are Paying For California’s Illegal
Aliens’ Health Care
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Monday, March 24, 2025, 10:03
AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-011:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
What Potential Federal Medicaid Cuts Could Mean for
States and Their Residents
-
Wave of long-term care insurance claims growing
faster than age wave, expert says
-
The Big Secret About Medicaid: It’s a Middle-Class
Benefit
-
MedPAC Members Will Hear Out Agents, Brokers After
Slamming ‘Flawed System’
-
California’s Medi-Cal shortfall hits $6.2 billion
with ‘unprecedented’ cost increases
-
U.S. Short-Term Care Insurance Market to Reach
$110.1 Billion by 2033 | Persistence Market Research Report
-
American Voters Want Commonsense Medicaid Reforms
-
Opinion: Households [sic] plans for long-term care,
but those plans may not reflect reality
############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Friday March 21, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC
BULLET: ILTCI ’25 VIRTUAL VISIT
LTC Comment: ILTCI ’25 was another
successful industry convocation. Your “virtual visit” to the conference
follows the ***news.***
*** 3/6/2025, “Milliman’s
annual U.S. industry LTCI claims projection,” by Rachel Marsiglio,
Juliet Spector, and Robert Eaton, Milliman
Quote: “Long-term care insurance (LTCI) is almost 50 years old.
In the 1990s, more than 100 companies were selling policies to individuals
and to groups. In 2003, the pattern of annual increases in sales came to
an abrupt end and LTCI policy sales began to decline rapidly. Between 2003
and 2009, individual policy sales declined by 9% per year. Fewer than 15
carriers remain in the market. As the U.S. population ages, the
market for hybrid life and LTCI policies has been growing. In addition, we
see new standalone LTCI products filed in 2025 from insurers that had
previously ceased most sales.”
LTC Comment: Click through for fascinating details including “the
expected benefits (paid claims) that long-term care (LTC) insurers will
provide over the remaining life of the policies as of year-end 2023.” ***
*** TWILIGHT WISH: Every year the
ILTCI Conference supports a charity by donating funds and matching
attendees’ gifts.
Twilight Wish was this year’s recipient. Twilight Wish Foundation is a
nonprofit organization dedicated to granting wishes to seniors aged 68 and
older who live at or below the poverty level or reside in nursing
facilities. Their mission is to honor and enrich the lives of deserving
seniors through wish-granting celebrations that connect generations,
aiming to make the world a "nicer place to age, one wish at a time." ILTCI
reminds attendees: If you forgot to donate, or attempted to donate to
Twilight Wish Foundation but experienced some internet issues, please use
the link below to donate to this year's charity Twilight Wish so we can
support the amazing work they do! Donate
here.” I’m sure contributions from non-attendees would be equally
welcome. ***
*** ILTCI CONTEXT: For the history of
long-term care insurance conferences through 2021, go
here. But that’s 80 pages, so for a quick overview and analysis, check
out this ten-minute “podcast.”
If you’d like to see our most recent virtual visits to ILTCI conferences,
go
here for 2023, and
here for 2024. ***
LTC BULLET: ILTCI ’25 VIRTUAL VISIT
LTC Comment: The 2025 Intercompany
Long-Term Care Insurance Conference convened March 9-12 in Philadelphia at
the Marriott Downtown. This year’s theme was “Getting Stronger.” Over 1000
registrants participated representing all aspects of the LTCI business and
related fields.
This “virtual visit” to the conference
is intended to give those who were unable to attend, especially the LTC
insurance producers doing the hard sales work out in the commercial
trenches, some idea of the content and mood of the meeting.
Exhibit Hall Opening Reception
The opening reception, Sunday night,
March 9, was an excellent kick off. Free drinks and ample food sparked
conversation and networking between participants, and with exhibitors and
sponsors. Philly cheesesteak sandwiches, mussels in a garlic butter sauce,
and a wide selection of Mediterranean food pleased palates.
Opening Session
The opening general session led by
conference chair Jeff Levin of OneAmerica, began at 8am Monday morning,
March 10, immediately after an excellent buffet breakfast. Levin
recognized former leading lights of the industry by name and talked about
how LTCI has grown, shrunk, and expanded again, getting better all the
time. This year’s program included 219 speakers, 34 sponsors and 49
exhibitors. Mr. Levin observed that volunteers make the meeting happen and
he recognized them. He graciously thanked conference staff Diane Fulton
and Christi Trimble for their organizational work. This year ILTCI
partnered with Twilight Wish, a charity to make wishes come true for
seniors. ILTCI matched contributions to the charity by conference
attendees. A drawing for a $1,000 gift card was in play for attendees who
filled their “bingo cards” with stamps from each of the exhibit hall
booths.
After Conference Chari Levin announced
that Gina Betz of illumifin will be next year’s conference chair, she
invited everyone to ILTCI ’26 that will be held in Orlando, FL at the
beautiful Rosen Shingle Creek Resort, about which a marketing video for
the property teased audience interest.
Next came the announcement of this
year’s
ILTCI Recognition Award recipients. Carroll Golden, Executive Director
of NAIFA Specialty Centers and Denise Liston, Senior VP at illumifin
received the honor this year. Both delivered thoughtful remarks in thanks
for the recognition, the trophy and the honorarium. They join a proud
group of former award recipients including Marc Cohen (2018), Stephen
Moses (2019), and Ron Hagelman, Peter Goldstein and the company LTCI
Partners (2024, after a five year hiatus without the award being granted).
Keynote Speakers
This year’s “keynote address”
followed. It was unique. Instead of the usual motivational speaker, we
were presented a series of video clips from a forthcoming Public
Broadcasting System documentary highlighting the challenges of caregiving.
The two-hour program,
Caregiving, will air on 330 PBS stations across the country
in June. Care Scout sponsored the keynote and CEO Samir Shaw introduced a
panel of speakers who discussed the origin, planning and challenging
creation of the program. This groundbreaking public media documentary
delves into the personal stories of caregivers, shedding light on the
challenges they face in providing short and long-term care, as well as
palliative and end-of-life care for individuals of all ages. The
four-person panel representing creators of the documentary and including
one caregiver, whose story was especially moving, described how the
program was conceived, how caregivers willing to tell their stories were
found, and how they completed the project.
In the Q&A session that followed, the
panel was asked how many of them own LTC insurance. Answer: Not one. That
admission revealed the LTCI industry’s fundamental challenge, getting
people, even those touched by the challenge of caregiving, to take
concrete measures to prepare for the risk and cost of needing care one day
themselves. On that issue, I have something to say in the Closing LTC
Comment below.
Breakout Sessions
This year’s breakout sessions were
presented in seven substantive tracks: Advisors, Agents, & Agencies;
Actuarial & Finance; Claims & Underwriting; Legal, Compliance &
Regulatory; Marketing, Engagement, & Research; Management & Operations;
and Wellness & Aging in Place Solutions. Following are summaries of each
of the breakout sessions I attended.
10:45am, March 10: “How Can
Behavioral Economics Change LTCI (For the Better)?”
Marketing, Engagement, & Research Track
Moderator: Jodi Anatole, Endeavour
Consulting
Speakers:
Andy Freedman, Assured Allies
Richard Mathera, Irrational Labs
Monika Shvetz, Mindful Marketing Solutions LLC
Session description:
Behavioral economics combines elements of economics and psychology to
understand how and why people behave a certain way - and can be used to
change behavior to create better outcomes. Learn the principles of
behavioral science, examples from other industries, and how they can be
applied to improve the experience for LTCI - for carriers, producers, and
policyholders. Specifically: How do you capture attention and motivate
people to make decisions? How do you communicate more effectively? What is
the reaction when something doesn’t cost anything? What is a “Nudge”? And
ways to adopt this concept into what we do. This will be an interactive
session where the audience will have a chance to pose their challenges and
experiences where adoption of behavioral economic principles have made an
impact.
LTC Comment:
I found this session fascinating. Richard Mathera explained the
many ways people behave irrationally and how to recognize and adapt to
those human foibles. Bottom line: Design for clients’ unique needs; reduce
uncertainty. That’s how to think about behavioral science. Freedman of
Assured Allies explained how his company employs behavioral strategies
to help LTCI carriers reduce risk, bring solutions to policyholders, and
help people stay at home longer. Behavioral insights helped his company go
from “asking people to contact to us to concentrating on specific
challenges like how to get dressed.” Monika Shvetz focused on
behavioral psychology in advertising. She said “Know your customer is Rule
1. Rule 2 is you can’t be everything for everyone. Develop “mindful
marketing strategies.”
2:00pm, March 10: “The Heavyweight
Champions of LTC Planning Strategies”
Advisors, Agents, & Agencies Track.
Moderator: Elena Castor, AdvisorEdge
Solutions
Speakers:
Zack Derryberry, ACSIA Partners
Jamie Mueller, OneAmerica Financial
Shawn Britt, Nationwide
Session description:
Sit ringside for an exciting exhibition of Advanced LTC Planning
Strategies. This three round event will spotlight the successful use of
IRAs and Qualified assets in LTC Planning, Pension Protection Act (PPA)
Qualifying LTC Annuities, and Small Business Owner and Carve-Out Planning.
Tax savings and LTC planning are the ultimate ‘one-two’ punch combination;
together they’re a knockout. See how these strategies incorporate
protection and tax savings to produce 2X the planning value for your LTC
prospects while opening an entirely new LTC premium resource.
LTC Comment:
This session was a revelation to me. I had no idea how vital tax planning
is to LTC financing strategy. Mueller from OneAmerica explained how
non-qualified annuities and the Pension Protection Act “let us help people
with these widely owned annuities.” ACSIA Partners’ Derryberry
focused on how IRAs and Qualified Assets magnify the benefits of planning
for LTC. He observed that, ironically, the SECURE Act may create greater
taxation for an IRA beneficiary than if funds were withdrawn by the
original IRA owner. “Using qualified assets and IRAs for premium dollars
can be a more efficient IRA distribution strategy compared to ‘defer and
die’ where the IRA is transferred at death.” Shawn Britt of Nationwide
explained the tax advantages of long-term care insurance for Business
owners and employees. She showed charts of allowable tax deductions by
decade of age. Use LTCI to “recruit, retain, reward.”
3:45pm, March 10: “Rumble in the
Breakout Jungle! Short-Term Care v. Long-Term Care”
Advisors, Agents, & Agencies Track.
Moderator: Stephanie Moench, Oliver
Wyman
Speakers:
Erin Bueltel, Wellabe
Corri Campbell, Mutual of Omaha
Kent Little, New York Life
Dennis Rinner, GoldenCareUSA an Integrity Company
Session description:
If they were boxers, the short-term care insurance industry and the
long-term care insurance industry would probably notice each other
training in the same gym. While they would likely be in slightly different
weight classes, they would share many of the same attributes, have similar
goals, and ultimately their personal battles would occur in the same ring.
As the extended care market evolves, the relationship between these two
competitors may be changing. Are the long-term care insurance and
short-term care insurance industries going to become sparring partners who
make each other stronger? Will they start to compete head-to-head more
often? Like Apollo Creed, will long-term care insurance be forced to
reckon with a scrappy, humble, and strong short-term care insurance
industry that has the potential for mass appeal? Or, like Rocky and
Adrian, will the two industries embrace, express their love for each
other, and walk hand in hand into the streets of Philadelphia? During this
session, we’ll go to the canvas with an excellent panel of insiders and do
a fresh weigh-in on these questions.
LTC Comment:
As the session description explains, this program compared the roles,
strengths and weaknesses of short-term care insurance (STCI) vs. long-term
care insurance (LTCI). Moderator Moench of Oliver Wyman clarified
key differences between STCI and LTC, such as STCI covers no more than
360 days and is often employed as gap coverage for Medicare. Presenters
discussed the question “Can STC and LTC co-exist?” They observed that it
is more important to talk about goals and solutions, rather than about
types of insurance. STCI can be an alternative for LTCI declines. Most
people think of STCI as short term health insurance. It is not short-term
major medical. LTCI’s Achilles’ Heel is affordability. The more options
producers and prospects have, the better. There is an option for
everybody. STCI is not available in every state. Compared to questions
that really matter; the choice between STCI or LTCI is not one of them.
9:00am, March 11: “Innovation in
Long Term Care Insurance – A Regulatory Perspective”
Legal, Compliance & Regulatory track.
Moderator: Nolan Tully, Faegre Drinker
Speakers:
Shannen Logue, Pennsylvania, Department of Insurance
Ben Veghte, Washington State Department of Social and Health Services
Tomasz Serbinowski, Utah Insurance Department
Session description:
This session will be a moderated panel discussion focused on putting
forward the regulatory viewpoint on various existing and future
innovations in long term care insurance. What do key regulators think
about pre-claim wellness programs, new products aimed at continued
engagement with policyholders, opportunities that might come from state
based public insurance programs and other cutting-edge issues? Come to
this session to find out!
LTC Comment:
Shannon from PA-DOI opened the discussion with a poignant
observation: after all these years, we’re still talking about same
problems, such as affordability; new products, high care costs, adding
LTCI to this, that and the other thing. Tomasz from the Utah ID
observed that regulators are not natural innovators so this is not a
natural place to look for innovation. That comment encapsulated my
impression of this session. The old questions about how to reach the
middle market; the regulatory quagmire; the fruitless search for a
government program to solve all; and the unsatisfying fall back to
identify a public/private combination; all these signal the absence of
innovation. Veghte from WA Cares represented the best this kind of
thinking can deliver, one more example of a compulsory, payroll-funded,
centrally planned, dubiously financed entitlement program. Innovation is
needed, but it does not look like we should expect much of it from
regulators or government bureaucrats.
10:45am, March 11: “Thinking in the
Middle: How do we serve the Underserved Middle-Income Market?”
Marketing, Engagement, & Research Track
Moderator: Eileen Tell, ET Consulting,
LLC
Speakers:
Liz Christofer, HCG Secure
Chris Giese, Milliman, Inc.
Beth Ludden, CareScout
Dustin Plotkin, Oliver Wyman
Session Description:
After decades of product innovation and industry effort, LTC insurance
still remains a product largely purchased by a small segment of the more
affluent Americans. There is large untapped market potential and great
need for financial protection among the middle-class. Using data from a
recent survey of middle-income consumers, this session will shed insights
on the size and nature of demand of LTC coverage within this market
segment, discuss some of the barriers to purchase and ways to overcome
them. After a brief panel discussion, the audience will get creative and
help evaluate, reject, or re-design four new product prototypes intended
for appeal to middle-income consumers.
LTC Comment:
Surveys to understand the LTCI middle market relative to the affluent
market show, no surprise, that affordability is key. They indicate better
education is needed. Middle income people are less likely to save or
insure for LTC than others who are more prosperous. Two reasons: lack of
awareness and misunderstanding. They are less likely to believe they will
need LTC one day. What might incentivize the middle class to take LTC more
seriously? The most important incentive is financial benefits. Middle
income people place a high value on advice from personal advisors. So,
bring financial advisors more into the mix.
After the opening general discussion,
this session broke into smaller work groups to consider and evaluate
different product models in terms of how they might behave given the
challenges and concepts identified in the general session. I missed this
portion of the program due to a previously scheduled networking
appointment.
My impression is that experts have
studied LTCI buyers and non-buyers six ways to Sunday for decades. What
they rarely explore is the market context in which LTCI sales occur. That
market is dominated by the primary LTC payers, Medicaid (44%) and Medicare
(16%). Without addressing those elephants in the room, all the detailed
research and analysis lead nowhere, beyond being very interesting and
stimulating intellectually.
2:00pm, March 11: “Carrier
Perspective: The State of our LTC Industry”
Marketing, Engagement, & Research Track
Moderator: Ramona Neal, Living Benefit
Review
Speakers:
Joe Laskowski, CareScout
Scott Limes, Nationwide
MacKenzie Madsen, Lincoln Financial Group
Larry Nisenson, Assured Allies
Ryan Bivins, John Hancock
Brian Kendall, OneAmerica Financial
Session description:
State of the LTCi industry. Taking a macro view of our industry - where is
it today and where is it headed?
LTC Comment:
The panel included representatives of “pure,” traditional LTCI on the
left, mixed LTCI (hybrids) in the middle and mostly life insurance
products on the right. Moderator Neal complained “we need one name for the
middle category,” which she called “MoneyGuard” to some objection.
Larry Nisenson of Assured Allies had several observations about the
past, present and future of traditional LTCI. It’s left a “bad taste in
the mouth of clients and producers,” “has a history to overcome,” flagging
sales say it all. Wellness and annuities offer a path forward. “Innovation
is the root of all opportunity.” MacKenzie Madsen of Lincoln Financial
Group spoke about the evolution of the hybrid marketplace, starting 35
years ago with Golden Rule, then OneAmerica, looking for younger customers
and more affordability. The products need to simplify, offer more value.
Joe Laskowski from CareScout opined how career agents dominated
early on. Distribution is adapting away from “one size fits all” to
“bespoke” products fitting specific clients’ unique needs and preferences.
Brian Kendall of OneAmerica Financial observed “we have so many
ways now to meet needs. We need to be more open- minded to nontraditional
ways of doing things. Hear, hear!
3:45pm, March 11: “The Title Fight:
The Good, the Bad, and the Knockout AI Tactics to Boost Marketing,
Research, & Engagement”
Marketing, Engagement, & Research Track
Moderator: Winona Berdine, Continental
General
Speakers:
Emilie Ansel, Private Health News
Aashima Kapoor, Homethrive
Session description:
Participate in this this high-energy session where industry experts will
coach you on how to transform your business approach using real-world AI
tools and techniques. Learn how to work smarter, not harder, by making AI
the foundation of your strategies. Discover how to avoid reinventing the
wheel, how to ask the right questions (and what NOT to ask), how to tame
the skeptics, and tap into AI's potential to simplify marketing, enhance
content creation, and drive customer engagement. Whether you're new to AI
or looking to expand its use, this session will empower you with
actionable insights and takeaways to grow your revenue and audience
effectively.
LTC Comment:
This was a fascinating session unveiling a plethora of ways to put
Artificial Intelligence (AI) to work in our professional lives. For
example: using AI to answer questions for prospects and clients. Pointing
them to specific ways to fill their needs. Ask yourself: “Where am I not
using AI?” Then use it in those areas because AI is applicable virtually
everywhere. In terms of how to use AI; ask for exactly what you want;
provide context; give specific instructions; explain how you’d like the
answer printed out. The more guidelines you specify the better results
you’ll receive.
Here’s my two cents worth. I asked AI
to read my 80-page “History
of LTC Insurance Conferences,” summarize it, and present the results
in the form of an interview. It took Google Illuminate 30 seconds to
produce this 10-minute
podcast. As
Arthur C. Clarke said: "Any sufficiently advanced technology is
indistinguishable from magic."
Closing LTC Comment:
The most telling and unfortunate occurrence of ILTCI ’25 was when the PBS
producers of their moving story about caregivers acknowledged that none of
them owned LTC insurance. That put the conference’s main shortcoming into
stark relief. In none of the general and breakout sessions I attended, and
I expect in few if any of the sessions I missed, was attention given to
the broader market in which LTC insurance is sold. Medicaid and Medicare
dominate that market, but were barely mentioned. I heard nothing about how
easy access to Medicaid LTC benefits after care is needed anesthetizes
future generations to LTC risk and cost. This reality crowds out demand
from the same middle-market prospects LTCI marketers find so elusive. Nor
was there any focus on the needs of LTC providers, such as nursing homes,
assisted living facilities, and home health providers. They are desperate
for private financing sources that pay market rates to relieve their
excessive reliance on low Medicaid reimbursements that hamper care
quality. Until the LTCI industry wakes up and addresses these public
policy issues, no amount of surveys, focus groups, brainstorming, or
WISHful Thinking for an easy government solution will succeed.
Another reality I found unaddressed at
the conference was any recognition of the political and economic turmoil
going on in America right now. Whether you like it or hate the current
disruption, it is a time—the first time in at least two decades—when
substantive change to the policies and rules governing Medicaid LTC
eligibility and LTCI marketability is possible. Republicans want to cut
$880 billion from Medicaid. Democrats want to protect low-income
enrollees. Neither goal is wrong. Both are achievable. But not without
more creative thinking and stronger political advocacy. I proposed a way
to proceed in a recent column: “Disrupt
LTC Now.” I welcome your feedback at
smoses@centerltc.com.
#############################
Updated Tuesday, March 18, 2025,
10:03 AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-010:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Medicaid Improper Payments Are Not a Measure of
Fraud or Abuse
-
Life Insurance Products Could Slash Billions in
Government Spending, Report Finds
-
California Borrows $3.4 Billion for Medicaid
Overrun as Congress Eyes Steep Cuts
-
Medicaid’s True Improper Payments Double Those
Reported by CM
-
More Than Two-Thirds Of Women Investors' Careers
Impacted By Caregiving Responsibilities
-
California’s Insurance Tax Shuffle: How Federal
Money Ends Up Paying for Medicaid for Illegal Immigrants
-
Representatives reintroduce bills supporting
Medicare OT at home, long-term care catastrophic care fund
-
Milliman’s annual U.S. industry LTCI claims
projection
-
Do older adults understand healthcare risks?
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Monday, March 10, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC E-ALERT #25-009:
LTC NEWS AND COMMENT
LTC Comment: Do you spend hours searching
the internet for useful articles, key data, and relevant reports to keep
you on the forefront of professional knowledge? Do you lose business
because you’re blindsided by clients or competitors who learn critical
information before you do? Here’s an antidote:
LTC Clippings: The Center for Long-Term
Care Reform notifies subscribers to our LTC Clippings service daily of
information you need to know. Each message contains only the critical
facts about new publications: a title, representative quote, a link to
the original, and our analysis in a sentence or two. To inquire or
subscribe, contact Damon at 206-283-7036 or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC E-Alerts: Once a week, we compile our
daily LTC Clippings into a summary, email it to Center for Long-Term Care
Reform members, and archive it in The Zone, our password-protected
members-only website. Center members also receive our weekly LTC Bullet
op-ed. To join the Center and receive all these benefits and more,
contact Damon at 206-283-7036 or
damon@centerltc.com.
We no longer post our LTC E-Alerts on the
Center’s public access website, but here’s what today’s LTC E-Alert
contained: links, quotes and comments on the following articles, reports,
or data:
-
The EINSTEIN Option reimagines long-term care
-
illumifin CEO Peter Goldstein Joins Alzheimer’s
Association Board of Directors
-
Costs increase across long-term care in 2024, with
homemaker and assisted living taking lead, Genworth report finds
-
Genworth and CareScout Release Cost of Care Survey
Results for 2024
-
As baby boomers turn 80, there aren’t enough
doctors to treat ‘emergency levels’ of dementia patients
-
Alzheimer's May Develop Differently in Women
-
Is the ‘Age Wave’ a retirement tsunami? — With Ken
Dychtwald
-
Dementia risk in the U.S. after age 55 higher than
previously thought, study finds
-
California Has a Lot to Lose If Trump Slashes
Medicaid
-
How would Medicaid cuts impact seniors in nursing
homes?
#############################
"LTC E-Alerts" are
a
feature offered by the Center for Long-Term Care Reform, Inc. to members
at the $150 per year level or higher. We'll track and report to you news
and analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Friday March 7, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC
BULLET: LTCI CONFERENCES ILLUMINATED
LTC Comment: On the eve
of the 2025 ILTCI Conference, we celebrate the distinguished history of
long-term care insurance conferences, after the ***news***
*** DON’T MISS this
extraordinary AI-generated “podcast”
recounting the history of LTC insurance conferences. Click
here and listen to 10 minutes of commentary summarizing and analyzing
a quarter century of professional LTC insurance meetings. ***
***
ILTCI ’25 convenes in Philadelphia March 9-12. Attendees can access
the meeting’s mobile app
here. Directions to the
Philadelphia Marriott Downtown and parking information are available
here. If you haven’t registered already, do so
here. Hope to see you there. ***
*** 3/3/2025, “Genworth
and CareScout Release Cost of Care Survey Results for 2024,” Genworth
and CareScout
Quote: “The cost of long-term care services increased across all
care types, according to the 2024 Cost of Care Survey conducted by
Genworth and CareScout. While homemaker and assisted living community
costs increased the most at 10%, the increase for most care types
continued to outpace inflation.”
LTC Comment: Click through for the startling details and go
here for the full report. As we do every year, we’ve posted the annual
Genworth/CareScout LTC cost-of-care report in the Center’s members-only
website (The Zone) for easy access anytime. ***
LTC BULLET: LTC
CONFERENCES ILLUMINATED
LTC Comment: Today’s
LTC Bullet is our 1400th since the Center for Long-Term
Care Reform’s founding in April 1998. During those years we reported on
every major LTC insurance conference. In April 2021, in the throes of the
pandemic and shortly after a “virtual” conference replaced that year’s
cancelled in-person gathering, we published a “History
of LTC Insurance Conferences.” We encourage you to browse that history
and remember (for those who lived them) or learn (for those new to the
business) the extraordinary challenges, victories, defeats and progress
we’ve shared. While you’re at it, check out a few photos of LTCI leaders,
many of whom are still around, though maybe a little longer in the tooth.
To get you off to an
easy start, listen to this
10-minute interview, generated by
Google Illuminate, discussing the “History
of LTC Insurance Conferences.” I think you’ll agree it’s pretty
amazing what Artificial Intelligence can do in 30 seconds with an 80-page
document that could take you several hours to read carefully and many more
to analyze thoughtfully. See if you agree with the robots’ summary and
analysis.
For my part, I attended
and reported on almost every one of the LTC insurance conferences starting
in 1991. You can find the Center’s real time coverage of the meetings,
often called “LTC Embed Reports” or “Virtual Visits,” going back to
January 2000, by searching for the word “conference”
here. I watched the early “Private LTC Insurance Conferences”
gradually co-opted by advocates of public LTC financing and eventually
replaced by the Intercompany LTC Insurance Conferences (ILTCI) sponsored
by the Society of Actuaries and honchoed by Jim Glickman. Among my
favorite meetings over the years were the ones aimed at educating and
inspiring LTCI producers. Thank Jesse Slome and Greg Luque for making
those agent-oriented conferences happen. They’re included in the history.
I haven’t always been
thrilled with the LTCI conferences’ evolution. In the early years, they
took more notice of how private insurance fits into the broader LTC
industry. Efforts were made to reach out to LTC providers such as nursing
homes, assisted living and home care companies. There was great potential
in linking the interests of businesses that supply LTC insurance with
others that benefit from funding LTC privately. But that relationship
never matured. Nor did an early focus on understanding, adapting to and
changing public LTC financing policy for the better. After progress in the
Deficit Reduction Act of 2005 (a cap on Medicaid’s home equity exemption,
longer and stronger transfer of assets restrictions, and unleashing the
LTC Partnership Program), further Medicaid reform and stronger LTCI tax
incentives were never achieved. Nowadays, we see a very positive focus on
wellness initiatives, but otherwise the emphasis is on technical issues
and marketing, important but not necessarily transformational topics.
Still, the surviving ILTCI meetings are a great place to meet, network,
and learn. Hope to see you in Philly.
To close, here are some
highlights culled from the “History
of LTC Insurance Conferences” selected for you by the Center’s Vice
President for Administration, Damon Moses. He’ll be in Philly too, so say
hello.
2001,
Miami, FL:
ILTCI #1
“John
Hancock featured a guest celebrity, knuckleball pitcher Phil Niekro,
signing baseballs for a line of fans stretching all the way out into the
hallway. CHCS had perhaps the most unique hospitality suite. They created
the illusion for each participant of an old age infirmity, such as smeared
glasses to imitate cataracts, and then in true Florida style, let them try
their luck at completing a punch card voter ballot with the correct
answers to a delayed word recall test.”
“Steve
Moses gave this talk [‘Long-Term
Care's Race for Survival’] to the First Annual Society of
Actuaries Intercompany LTCI Conference in Miami, Florida on January 23,
2001. In it, he summarizes the Center's recently published
LTC Triathlon
study. He diagnoses the malaise in America's long-term care service
delivery and financing system. And he makes an appeal for greater
communication and cooperation between the private sector financiers,
providers and insurers of long-term
care.
2002,
Beverly Hills,
CA
According to conference organizers: “A LONG, HARD LOOK at long-term care
insurance reveals a product on the cusp of widespread acceptance. However,
as LTCI has come of age, so too have the challenges facing insurers: the
internet's effect on underwriting, claims practices, pricing
assumptions, population eligibility,
profitability management, and legislative
initiatives, to name a few.”
2003,
Las Vegas, NV
Unless
LTCI specialists understand what nursing homes, home health companies, and
assisted living facilities are up against, they cannot fathom why LTC
providers (and the public) mostly ignore long-term care insurance and
cling to government financing alternatives. For example, the conference
offered no educational sessions on public policy, on long-term care
service delivery, on competition from the 800-pound gorillas of long-term
care (Medicaid and Medicare), on the Medicaid-driven
fiscal crisis
in the
state and
federal governments
which practically begs for
help from private
insurance, on
the drought
in debt
and equity
capital facing
long-term care
providers, nor on the huge tort liability and liability insurance
crisis facing LTC providers. …
“Monday, January 27,
2003: "Rate Stabilization -
What Does
it Mean
to Me?"
Moderated by David Benz of Thrivent Financial for Lutherans (see picture
below). Panel: Al Schmitz of Milliman USA; Peggy Hauser of the LTC Group;
and Dennis O'Brien of New York Life. This session anguished over rate
stability challenges: What went wrong? Why are rates going up?
How
can the
industry set
rates properly? What is
the proper
interaction between management,
actuaries and regulators? …
2003,
San Antonio, TX
The
16th Private Long-Term
Care Insurance
Conference: "Shaping the
Future." This meeting convened
at the Marriott Rivercenter Hotel in San
Antonio, Texas from February 12 to
14, 2003. The Private Long-Term Care Insurance Conference was the
grand-daddy of industry meetings in the LTCI field. Some say its name is a
misnomer, because this conference catered as much to advocates of
government long-term care financing as to manufacturers and purveyors of
private LTC insurance. People still complain about its 1993 conference in
Baltimore (during an ice storm) when Congressman Pete Stark bashed
long-term care insurance agents and insulted the industry in an
over-the-top "keynote" address. Check out all the details including many
contemporaneous pictures of LTCI’s leading lights in The Zone
here.
2003,
New Orleans, LA
The
National LTCi
Producers Summit
Presented by LTCi Sales Strategies
magazine, this 2½-day conference boasted a sold-out attendance of over 700
people, and featured 25 sessions, 50 LTC expert speakers, ample networking
opportunities, over
100 exhibitors, cocktail receptions,
breakfasts and lunches,
the LTCI Sales Idol contest, the top 10 producers contest, and even
optional sight-seeing tours.
The
Next Financial Boom: Reverse Mortgages & LTC Protection. Presented by
Peter Bell, President, National Reverse Mortgage Lenders Association,
Washington, D.C. In this session Peter
explained how
reverse mortgages can be
used as
an LTCi
financing sales strategy
to offer to prospects
that are house rich and cash poor.
The following are brief "man-on-the-street"
type of interviews. [Damon Moses] asked eight registered attendees two
questions: 1.) why don’t more people buy private long-term care insurance;
and 2.)
what percentage of total
nursing home
and home
health care
expenditures are paid
out of people’s assets (as opposed to any other source of funding, such as
Medicaid, Medicare, personal income, etc.)?
The
purpose of asking these two questions together is to illustrate one point:
that the majority of LTC services are not paid for by consumers, they are
paid for by the government. If a relatively small percentage of total
nursing home and home health care expenditures are paid out of people’s
assets, then why would the average person save for and then buy long-term
care insurance? Why would
people buy
something that
the government is giving
away? The
answer is that they
wouldn’t unless their assets were at risk. Here are the questions again:
1.)
Why
don’t more
people buy
private long-term care
insurance?
2.)
What percentage of total nursing home
and home health care expenditures are paid out of people’s
assets (as
opposed to
any other
source of
funding, such
as Medicaid, Medicare, personal
income, etc.) ?
To read these
interviews and see
the pictures
of interviewees,
check out
our
Virtual
Visit to this conference. [This content
is in the Center’s members-only content (The Zone.) You will need your
user name and password, for which contact Damon@centerltc.com.
2004,
Houston, TX
“The great thing
about this
conference is that
it brings
together all
components of
the long-term care
insurance industry in a setting that encourages cross training and mutual
understanding.
That's as opposed
to the
more adversarial
settings that
actuaries, marketing people, underwriters
and management often find themselves in, fighting to discover the right
balance between price and salability of a complicated, deeply conceptual
product.
“Unfortunately, there is a slight pall on the conference. Everyone knows
the long-term care insurance
industry faces
daunting challenges. In the
past years,
and especially
recently, we've seen consolidation, companies exiting the business, level
or declining sales, rate stability concerns, disappointing
profitability, etc. Industry analysts have painted a less-than-bright and hopeful picture of the business for the
immediate future. But, at least at this meeting, I find a strong
sense of
optimism and
renewed commitment that trumps
the downbeat
perspectives and worries.”
“A
long-term care
producer with
insight into
the back-office aspects of
the LTCi
business opined that
‘This industry has seen some hard times, but the worst is behind us.
Pricing is improving; public
awareness is
increasing; and
the same
promising demographics are still
out there.
Industry consolidation and belt tightening will prove to have been
healthy and beneficial in the long run.’
Steve Moses
made
the case
for private
LTC financing
while Dr. Judith
Feder, then
Professor and Dean
of Public
Policy at
Georgetown University appealed
for public
financing in
a session at
the Fourth Annual Society of Actuaries Long-Term Care Insurance
Conference in Houston, Texas on February 10, 2004.
2005,
Orlando, FL
“Today's
alert comes to you from the fifth annual Society of Actuaries Long-Term
Care Insurance Conference in Orlando,
Florida. The
SOA-LTCi meeting
has evolved
into the
premier industry event for executives involved in the nuts and
bolts of long-term care insurance. We realize many of you can't or won't
attend, so as we did last year from Houston, here's a brief report on the
proceedings from Steve Moses on site. …
LTC
Bullet: Clueless
in Orlando
2006,
Anaheim, CA
Attendees heard a report on the "Medicaid Commission’s” findings. Like
most commissions, it achieved nothing of consequence. Steve Moses
delivered a speech titled "What
I Believe About Long-Term Care." The Center's Vice President
for Administration, Damon Moses, circulated at the conference interviewing
attendees. Interview Question: What effect
do you
think the
new Deficit
Reduction Act
will have
on the
marketability of private
long- term care insurance? Can you put a percentage on that? Check
out our
Virtual Visit
for answers.
2007,
Dallas, TX
ILTCI #7 opened
to a
body blow
from the
New York
Times: “Aged,
Frail and
Denied Care by Their Insurers,” by
Charles Duhigg,
March 26, 2007. We responded immediately. Read our response and more about
this conference in our virtual visit titled
LTC
Bullet: Sucker Punched in Dallas,
Tuesday, April 10, 2007.
2008,
Jacksonville, FL
A
distinctive feature of this year’s conference was the presence, at the
venue’s front door, of a small Airstream trailer emblazoned with the
decals of companies sponsoring the Center for
Long-Term Care Reform’s 2008 “National
Long-Term Care Consciousness Tour.” Read all about
it in
LTC
Bullet: The
Jacksonville LTCI
Conference.
Enjoy this
musical
reminder
of tour highlights.
2009,
Reno, NV
The
Silver Bullet of Long-Term Care
again graced the entrance to the 9th Annual
Inter-Company Long-Term Care Insurance Conference. We published one
LTC Bullet
and three LTC E-Alerts (here,
here, and
here) about the meeting.
2010,
New Orleans
Gail Sheehy keynoted the
conference, but later dissed LTCI on NPR. Despite some very strong
panelists speaking on behalf of
logic, evidence and actuarial sanity (Steve Schoonveld of
LifePlans; Malcolm Cheung of Prudential; and Al Schmitz of Milliman), everyone
seemed to be bending over backwards to give CLASS the benefit of the
(clearly overwhelming) doubt.
2011,
Atlanta, GA
Four
breakout sessions focused on the CLASS Act including Steve Moses and John
Greene debating CLASS with Connie Harner and Rhonda Richards (AARP). Find
summaries of all four CLASS sessions and several other sessions in our
Virtual Visit to the conference
here. During the lunch break on the
second day, the
3in4 Need
More
campaign had a press conference to introduce the LTCI industry's answer to
dairy's "Got Milk" message. Spotted at the 3in4 Need More event and
throughout the ILTCI conference was Glenn Ruffenach of the Wall Street
Journal. Maybe there's hope for some good publicity for LTCI now.
2011,
Las Vegas, NV
Here’s another non-ILTCI conference to
remember.
The 9th LTC Insurance Producers Summit,
held April 3-5, 2011 in Las Vegas, had the theme "Get Over It!" Get over
lagging sales, disappearing carriers, premium increases, and bad
publicity. Get over it and, one might add based on the content of the
conference: Get On With It! Proceedings got underway with a
standing-room-only crowd for the "3 in 4 Need More" campaign's second
press conference.
Cameron Truesdell, CEO of Long-Term Care
Financial Partners, delivered the "Keynote Address." He pointed out the
desperate need for responsible long-term care planning and insisted: It's
up to us to make it happen. Echoing a patriotic appeal, he asked "If not
us, who? If not now, when?
2012,
Las Vegas, NV
For
a full account of
the conference’s
highlight event, the
“Clash of
Titans” debate between Harley Gordon and Steve Moses, check out
LTC Bullet: LTC Embed Report
from the ILTCI Conference in Las Vegas.
Now to
recount the most fun that was had at the conference. In the afternoon of
DAY ONE, a great debate ensued titled “Clash of the Titans:
Moses vs. Gordon on Medicaid and Other Dark Matter.” Ably produced and
moderated by
Federal Long-Term Care Insurance Program
CEO Paul
Forte, the
program included
a dramatic
“fight poster”
inviting the
audience to
attend, slides featuring great debates of the past, e.g.
Lincoln/Douglas, etc., and a dual-podium presidential-style debate format.
Moses and Gordon each began with 3-minute
opening statements. (Find a transcript of the “fable”
I began
with at
the end
of today’s
Bullet.) After
a coin
flip to
see who
would get
the first question, Forte
pummeled the combatants in turn with six queries ranging from why the
LTCI market languishes to what they’d advise presidential candidates to
say about LTC financing. Answers were strictly enforced to no more
than two minutes, with a one-minute rebuttal, and a final 30-second
“re-direct” by the original answerer.
The
program moved fast with lots of humor and more than just a little
gentlemanly confrontation. In the second phase of the debate, the
participants asked each other questions, with
the same
time limits
applying. Neither knew
what the
other would
ask so
the questions and responses were totally spontaneous. Finally, the
audience submitted written queries pinning down the debaters with new and
different viewpoints. Bruised, bloodied, but upright, Moses and
Gordon shook hands at the end and affirmed they remain friends. They look
forward to continue pursuing their different paths toward the common goal
to improve long-term care for all.
Who
won? Just
between you,
me and
the lamppost,
here’s how
LTCI producer
and author
Craig McCormick, a former college debater himself, scored
the matchup: 13 to 4, for Moses. Now, I acknowledge that Mr.
McCormick may have a bias in my favor. So I invite any of you faithful
readers out there who may have attended the debate to weigh in with your
own scoring of the event. I’d particularly like to hear from anyone who
gave the win to Harley instead of me.
Well, I want
to hear
from anyone
except you,
Harley! I’ll
publish any
thoughtful comments
or analysis of the debate in a future LTC Bullet. Let us
hear from you.
The
last session
I attended
was a
post-mortem on CLASS titled
“Meeting the
Needs that
CLASS Intended,” moderated by Prudential’s Malcolm Cheung
with presentations by Bob Yee, lately CLASS’s
actuary; Yair
Babab from
the University
of Illinois,
Chicago; and
Mark Meiners,
the father of the LTC Partnership Program. I came away convinced
less-than-ever that anything about CLASS is salvageable and more convinced
than ever that LTC financing solutions must come from reducing government
interference in the market, not increasing it. Stop giving away LTC to
people who should, could and would buy LTCI and the market will work its
magic.
2013,
Dallas, TX
Overall,
the mood of the conference was one of optimism and motivation. In
reference to this, Sally Leimbach states: “Several Exhibitors seemed to me
to be relatively small providers vying to become a part of the process of
underwriting LTCi or providing services at time of claim. To me,
that showed
optimism about
the growth
of the market among
providers.” Sally continues
by mentioning she encountered “[m]ore optimism than expected. It
rubbed off. I have come back reenergized
for educating
people to
plan for
LTC and
selling to
assist to
meet the
ever important need.”
What an excellent reminder of why events like this are so important to the
industry.
Many
conference attendees in Dallas expressed high satisfaction with the value
of networking opportunities with industry professionals as well as the
quality of educational content. Honey Leveen states:
For marketing people like me, the SOA [ILTCI
conference] is valuable. I gain insight into the LTCi product, its
actuarial, underwriting, and other elements I would otherwise not learn
about. I learn about the latest LTCi sales approaches, both from the
sessions and from colleagues. I learn about upcoming LTCi products.
Also, I get breaking news on LTCi national politics. I feel my
attendance at SOA conferences definitely gives me a competitive edge.
2014,
Orlando, FL
The
14th Annual
Inter-Company Long-Term Care
Insurance Conference
convened in
Orlando, Florida at the Rosen Centre Hotel from March 16-19, 2014.
We
asked conference
founder Jim
Glickman for his
highlights of
the meeting.
He responded:
1. The
14th Annual Intercompany LTCi Conference in Orlando, FL (co-sponsored by
the LTC Section of the Society of Actuaries) had over 900 attendees, an
all-time record surpassing the 855
attendees in Jacksonville,
FL in
2008. [NB:
the Silver
Bullet of
Long- Term Care was parked outside the conference venue in
Jacksonville as we were well underway with the Center’s 2008 “National
Long-Term Care Consciousness Tour.”]
2. As
usual, the largest representation from the 10 tracks (Actuarial, Claims,
Compliance, Field Marketing, Group, Home
Office Marketing,
Management, Operations, Policy
and Providers, and Underwriting) was from Field Marketing, followed
closely by Actuarial and then Management).
3. For
the first time in several years, there were attendees from multiple
insurance companies not
currently participating in the
LTCi marketplace,
together with
most of
the larger companies, who have at least temporarily, stepped away
from issuing new business.
4. Also
in attendance
were several
reinsurers not currently
in the
LTCi marketplace
together with several representatives of the private equity world,
apparently looking for new opportunities to consider.
5. The
two full
days and
two half
days featured
over 45 educational sessions,
together with more than
20 hours of organized networking.
6. The
Exhibit Hall
featured 54
Exhibitors, displaying all the
latest innovations
for insurance company home offices and their agents.
2015,
Colorado Springs, CO
The 15th
annual Intercompany Long-Term Care Insurance Conference convened March
22-25, 2015 at The Broadmoor resort in Colorado Springs, Colorado. The
annual Inter-Company Long-Term Care Insurance Conferences are always
something special. But this year’s meeting exceeded all that came before.
It exceeded by breaking past records: over 1100 attendees, up from the
900s; 72 vendors, up from 56; 44 sponsors and 170 speakers. It exceeded by
offering new programs including: demonstration rooms
where exhibitors could make
scheduled presentations; a
“social media”
room with
Twitter feeds; a “future leaders” program; a new Sales and
Distribution combination track; and a new “Alternative
Solutions” track,
honchoed by
Eileen Tell
and John
O’Leary, which
replaced Policy and
Providers, and captured me for all seven break-out sessions on the agenda.
2016,
San Antonio, TX
The
conference’s closing general session was It's Not Me, It's You; A
Consumer View on LTCI.
Behavioral economist Jeremy Pincus and
consumer insight
expert Luisa
Uriarte delivered new information about
how our
current approach
and sales
and marketing
techniques are
actually standing in the way a broader appeal for long-term care
insurance. These fascinating presentations challenged everything we
thought we knew about LTCI marketing, such as-- explain the problem, price
the risk, scare the pants off ‘em and they’ll buy. Well, no, turns out
that just drives people away. What’s needed is an approach that generates
good feelings and makes people positive about preparing for what’s coming.
Interestingly, this session was a perfect bookend for the conference, by
providing evidence from
behavioral research for some of the
same insights
about human
behavior shared
by the
opening general
session speaker
about the turnaround he
led at Harley Davidson.
2017,
Jacksonville, FL
THE 17TH
ILTCI CONFERENCE convened March 26-29 at the Hyatt Regency in
Jacksonville, Florida, with the theme “Navigating the Future.” What
follows are some quick impressions of the sessions I attended. These are
not a representative sample of the conference content as I visited
almost exclusively the program’s
“Alternative Solutions” track. Special
thanks to
Eileen Tell and John O’Leary for the hard work they expended to put
together the sessions comprising the Alternative Solutions Track. The
other tracks were Actuarial & Finance; Claims & Underwriting;
Combination Products; Legal, Compliance & Regulatory; Management,
Operations & Technology; and Marketing & Distribution. The conference also
featured a vast exhibit hall and special “demo rooms” where
companies could present their products and answer questions.
This year’s keynote
speaker, sponsored by Genworth,
was
Anat
Baron, former head
of Mike's Hard Lemonade,
a change strategist and “disruptor.” Her bio calls her a “force of nature”
and states “she spent her illustrious career moving at warp speed while
shaping and defining the trends that form today's business world.” She
turned around Mike’s Hard Lemonade by aiming its marketing at
women who
wanted something
to drink
out of a bottle
while guys
were quaffing beer. Her
message to the LTCI industry? “Disrupt or Die: Reinvention in an Ever
Changing World.” We live in a time of huge and rapid change. Facebook,
Twitter, Skype, the Cloud, etc., are
barely a
decade old.
Yet they’ve
changed the
world and
how we
survive, prosper
or not
in it. Social networking
rules. Master it or expect failure and embarrassment (such as being
identified in the audience as a flip-phone user or a non-texter.)
Ms. Baron’s session was entertaining and interesting,
but would have benefited from
more effort on her part
to apply her observations and
analysis to the LTC insurance business and its challenges.
2018,
Las Vegas, NV
The
18th Annual
Intercompany Long-Term Care
Insurance Conference was
held March
18-21, at the Paris
Hotel & Casino in Las Vegas, NV. Attendance was high at over 1,000
attendees, 60+ exhibitors and nearly 40 sponsors.
Every year the
Intercompany Long-Term Care
Insurance Conference takes
the pulse
of the
LTCi industry and offers direction forward. To that end, “A Matrix
of Opportunities” was the tagline for this year’s conference and that
optimism filled the agenda. According to the conference website’s
homepage:
A quiet
revolution is taking place in the long-term care insurance industry.
More interest than ever
is being
focused on
private sector
solutions to
the growing
societal issues
pertaining to long- term
care. Planning choices for consumers are growing at a rapid pace.
Insurance companies are developing
new innovative approaches to
providing long-term care
liquidity at various
life stages and
insurance agents and
financial advisors
are showing
renewed interest
in talking
to consumers about their
long-term care planning needs.
With
entitlements and social programs strained, longevity and healthcare costs
increasing, caregiver supply
decreasing and
the age
wave cresting,
how we
finance long-term
care now
and in the future is a demographic, political and fiscal Rubik's
Cube. This year’s ILTCI conference contributed
to solving
that multi-dimensional
puzzle by
hosting the
innovators who
are offering new
directions and products designed to save people from the risk and cost of
long-term care.
2019,
Chicago, IL
The
19th Annual
Intercompany Long-Term Care
Insurance Conference
convened at
the Sheraton Grand Hotel
in Chicago, Illinois from March 24 to 27, 2019. Today’s LTC Bullet
offers you a virtual visit to that event, the biggest of its nearly
two-decade history.
My
Million Dollar Mom, about Ross Schriftman’s movie he wrote and produced
about caring for his mother through her Alzheimer’s Disease.
First order of business was presentation of
the “ILTCI
Recognition Award” to “a person(s) or organization that has
made a significant, long-term contribution towards the attainment of the
ILTCI vision” which is “to create an environment for aging in America that
includes thoughtful, informed planning that takes into account the most
effective and efficient use of resources in addressing
the risks
and costs
of long
term care
for all
levels of
American society.”
Steve Moses, president of
the Center for Long-Term Care Reform, acknowledged the honor saying
I
like to think my stuff is kind of edgy, so I was afraid the ‘boos’ might
overwhelm the cheers after this announcement, but they didn’t, so thank
you. I want to thank the nominators, the board for selecting me, all our
wonderful friends and financial supporters. There are too many to list, so
I’ll only mention one by name, my son, Damon, whom many of you know. I’ve
heard this honor called a “lifetime
achievement” award. That
sounds like
you’re putting
me out
to pasture. So, to my friends, let me assure you I’m not going
anywhere. To those who disagree with me, don’t think this will stop me.
Thanks again to all.”
Tue, March 26th,
7:30 PM - 9:00
PM
Whirled
News Tonight
Improv
Show
General Conference Session
Our
Tuesday evening entertainment will feature performers from Chicago’s Best
Improv Comedy Theater – Improv Olympic! Improv Olympic will be bringing a
seven person cast of performers to entertain the attendees of the ILTCI.
The performance will be approximately 60 – 80 minutes in length. “ iO” is
recognized as the birthplace of
“long-form” improv and is home to some of the best improv comedy shows in
the country. They have helped to train and develop an entire generation of
America’s best and brightest comedic entertainers for over 30 years.
Alumni include past and present cast members of Saturday Night Live and
stars of some of your favorite small screen prime-time comedy and
late-night shows – along with others who have gone on to write, direct and
produce blockbuster Hollywood movies. This interactive show will include
performance pieces
including musical games,
scenes that
solve the
audience’s problems and
their signature piece, THE DREAM, based on the day in the life of
one of the audience members. To learn more about iO, visit https://www.ioimprov.com/
It will be a improve show of Olympic proportions…we hope to see you there!
LTC
Comment: And a
good time
was had
by all
at this
closing session
of the
conference. Stay tuned
to LTC Bullets for information about the 20the ILTCI Conference in
Denver, Colorado March 29 to April 1, 2020 as it becomes available.
2020: Cancelled because of the pandemic
2021
LTC BULLET: 2021 ILTCI VIRTUAL CONFERENCE WRAP UP
LTC Comment: The 2021 Intercompany Long-Term
Care Insurance (Virtual) Conference is history. Organizers Barry Fisher
and Vince Bodnar eased potential participants into the idea of a virtual
conference with
weeks of
advanced notice
and guidelines.
They recruited
sponsors for the overall
meeting, for each track and even for each session. Virtual
exhibitors
were encouraged to sign and pay up. Somehow, Fisher and Bodnar
managed to fund the effort, because beginning Tuesday, April 13, 2021, it
kicked off successfully.
After an
Opening General Session on the 13th, two different educational
sessions began on the hour each
Tuesday and
Thursday for
three weeks
from 12pm
– 4pm
EDT and
ran for
50 minutes each,
followed by 10-minute breaks. Find the agenda
here. Sessions were recorded and are
available to any and all through June 2021 using the password ILTCI*2021.
Here’s how to
access those
recordings: Open
the ILTCIConf.org screen. Click
“Schedule” on the navigation bar
at the top of the page. Click the track name of the session you want to
watch. Then find
and click
the session
you’re looking
for in
the list
of track
sessions. Find
and click
the “Access Recording” button at the bottom of the session
description. Fill out the information to identify yourself, click “I am
not a robot” and you’re in … hopefully.
As might
be anticipated with a complicated virtual conference, the outcome was not
electronically flawless. The opening session was to be a talk by futurist
Anders Sörman-Nilsson,
who was actually in Australia speaking at 2am local time the next day.
Interruptions and sound difficulties
caused that
session to
be cancelled
in the middle, but
organizers expect a
recording of it, done without the long-distance complications, will be
available.
Session
Title: The
WISH Act:
Addressing the
Financing and
Regulatory Needs
Within LTC
Public/Private Solutions
Track: Legal,
Compliance, &
Regulatory
Presenters:
Peggy
Hauser (PwC),
Steve
Schoonveld
(Moderator, Lincoln
Financial Group),
Tom Suozzi
(NY State)
Comments: This
session discussed the implications
of a
proposed federal
catastrophic long-term
care program, the WISH Act. The session focused on the benefit to
consumers, the financial soundness of the proposed program and the
regulatory steps necessary to achieve the desired public/private insurance
program goals.
#############################
Updated Monday, March 3, 2025, 10:03
AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-008:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Older households at risk of not being able to
afford long-term care, analysis finds
-
Unum Finds Reinsurer for Block of Individual
Long-Term Care Policies
-
Generation X is ready for senior living. Here’s
what they want
-
Why the Medicaid 'chainsaw' will come for your home
-
Disrupt LTC now
-
Capping Per Enrollee Spending Could Reduce Federal
Medicaid Expenditures by $532 billion to Nearly $1 Trillion Over 10
Years Depending on How States Respond and Result in as Many as 15
Million People Losing Medicaid Coverage by 2034; Eliminating the
Medicaid Expansion Match Rate at the Same Time Could Push Federal
Medicaid Spending Declines to as Much as $2.1 Trillion and Cause 30
Million to Lose Medicaid Coverage
-
Medicaid’s Cost Growth + Trump Health EOs
-
GAO’s High Risk List Highlights Ways to Save
Billions and Help Agencies Work Better
-
Is The American Dream In Crisis?
-
Stressed and confused, the new normal
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Monday, February 24, 2025,
10:03 AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-007:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Residents to recover 25 percent of entrance fees as
judge approves $86M sale of bankrupt CCRC
-
Trump Opponents Get Ready to Pounce on Medicaid
Cuts
-
House budget resolution could cut up to $880
billion in Medicaid
-
100-year lives – how age impacts the insurance
industry
-
Nursing home quality ratings drop after new
measures revealed
-
Young-onset dementia surges from 1990 to 2021
globally, data shows
-
10 Things to Know About Medicaid
-
US healthcare spending hits record highs, led by
senior care costs
-
What Recent Changes In MA Mean For Affinity Plans
And Supplemental Benefits
-
Retirement Community Living: How to Pay for Your
Next Chapter
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Friday February 21, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC
BULLET: LTC CENTER STANDING GUARD, NOW MORE THAN EVER
LTC Comment:
The current turmoil in U.S. politics and economics has made change for the
better more hopeful than in the past two decades. Some ways we’re helping
to improve LTC financing policy, after the ***news.***
|
*** TODAY'S LTC BULLET is sponsored by Claude
Thau (BackNine Insurance). BackNine gives you a free
personalized website at no cost. Your clients (& family & friends)
can, with as little or as much of your involvement as you or they
want, buy life insurance and LTCi, and can speed issue by scheduling a
paramed and uploading medical records immediately. We quote
stand-alone LTCi, linked-benefit and life with a LTC rider
side-by-side. Claude is the lead author of Milliman’s annual Broker
World LTCi Survey & a past Chair of the Center for Long-Term Care
Financing. Contact him at 913-707-8863 or
claude@back9ins.com to learn about more
great BackNine features and services. *** |
*** THE 2025
ILTCI CONFERENCE session matrix is now
available online! The Mobile App sponsored by Nationwide just went
live also. Attendees will have received a notification on how to download
the app and use its networking features. The meeting convenes March 9-12
in Philadelphia. Register
here. Book lodging
here. See you there! ***
***
GOOGLE ILLUMINATE is a program that can take an online document and
turn it into a podcast. I experimented by asking Illuminate to analyze and
report on “LTC Bullet:
So What If the Government Pays for Most LTC, 2023 Data Update” that we
published January 10, 2025. Check out the six-minute result by double
clicking
here. I expect listeners will find the result as illuminating or more
so than reading the original Bullet which was full of data and
technical analysis. ***
LTC BULLET: LTC
CENTER STANDING GUARD, NOW MORE THAN EVER
LTC Comment:
The Center for Long-Term Care Reform will celebrate the start of our 28th
year in April. In that quarter century plus, we’ve analyzed, criticized
and rebutted just about every study, report, article or commission that
attacked private funding or promoted compulsory government financing of
long-term care. We’ve identified ideological bias by scholars, think
tanks, government agencies, advocacy organizations and the media. We’ve
denounced their confirmation bias when they ignore evidence contradicting
their preconceptions. We’ve refuted fallacies in their logic. Today’s LTC
Bullet includes links to 119 LTC Bullets we’ve published taking
these groups and individuals to task:
Media: Consumer
Reports, National Public Radio (NPR), Public Broadcasting
System (PBS), New York Times, Wall Street Journal, Washington
Post, Dow Jones MarketWatch, Health
Affairs, National Affairs
Organizations: National Academy of Elder Law
Attorneys (NAELA, Medicaid planners’ trade association), AARP, Alzheimer’s
Association, Leading Age (formerly American Association of Homes and
Services for the Aging, LTC provider trade association)
Think
tanks or companies: Kaiser Family Foundation (KFF),
Georgetown Long-Term Care Financing Project, Urban Institute, Avalere,
SCAN, Employee Benefit Research Institute (EBRI), Bipartisan Policy Center
(BPC), Center for Retirement Research at Boston College, LTC
Collaborative, Milken Institute, American Enterprise Institute, AI
(Artificial Intelligence)
Government Agencies, Commissions and Politicians:
Government Accountability Office (GAO), the Medicaid Commission, the
Long-Term Care Commission, Congressional Research Service (CRS),
Congressional Budget Office (CBO), Medicare Trustees, Centers for Medicare
and Medicaid Services (CMS), Washington State’s “Long-Term
Services and Supports Trust Act (Trust Act),” Medicaid and CHIP
Payment and Access Commission (MACPAC), Representative Thomas Suozzi
(D-NY), WA Cares Fund and Washington State politicians, Medi-Cal and
California Governor Newsom
Scholars: Ellen O'Brien, Peter Kemper, Harriet
L. Komisar, Lisa Alecxih, Timothy Waidmann, Korbin Liu, Judith Feder,
Richard W. Johnson, Joshua Wiener, Mark Merlis, Lee Shirey Thompson, Anne
Tumlinson, Christine Aguiar, Molly O'Malley Watts, Diane Rowland, David G.
Stevenson, Marc A. Cohen, Janemarie Mulvey, Sudipto Banerjee, Richard G.
Frank, Neale Mahoney, Howard Gleckman, Leora Friedberg, Wenliang Hou, Wei
Sun, Anthony Webb, Gretchen Jacobson, Shannon Griffin, Tricia Neuman,
Karen Smith, Norma B. Coe, Melissa M. Favreault, David C.
Grabowski, Stephanie Kelton, Stuart Butler, The InLTCgentsia and
The LTC Anointed, Robert P. Saldin, Laura Benzing, Hannah Godlove, and
Megan R. Burke, Eileen Tell.
LTC Comment:
Speaking truth to power is a mostly thankless job. Please review the
efforts we’ve made to correct attacks on you for supporting responsible
long-term care planning. Browse the following LTC Bullets’ titles
and teasers. Pick a few to download and read in full. Then, if you find
value in our work, please support the Center for Long-Term Care Reform by
becoming a member or making a contribution. Become a member
here or contact Steve at smoses@centerltc.com or
425-891-3640 or Damon at
damon@centerltc.com or 206-283-7036 to join our fight for rational
long-term care financing policy.
LTC
Bullets Standing Guard
(The following Bullets are
listed in descending chronological order beginning with the most recent.
If you prefer to start from the beginning, just scroll to the bottom and
work your way back up.)
LTC Bullet: LTC Data Manipulation II,
January 27, 2025
LTC Comment: “Statistics don’t lie, but liars use statistics.” Still!
LTC Bullet: Catastrophic LTC Irony,
October 25, 2024
LTC Comment: Another report insists we need a big new federal program to
cover catastrophic LTC costs. Ironically, we already have one that makes a
new one impossible to achieve. We explain.
LTC Bullet: More KFF Data Misinformation,
September 13, 2024
LTC Comment: Does KFF misunderstand, misinterpret, or misrepresent LTC
insurance data? All three? See what you think.
LTC Bullet: LTC Data Manipulation,
August 30, 2024
LTC Comment: “Statistics don’t lie, but liars use statistics.” We explain
how KFF distorts National Health Expenditure data to promote ideological
conclusions.
LTC Bullet: There Is No “LTSS Gap”,
August 9, 2024
LTC Comment: This Health Affairs article offers a solution without
a problem. We provide a rebuttal.
LTC Bullet: KFF Hoisted Again,
June 28, 2024
LTC Comment: A series of KFF “issue briefs” intended to show how poor
Medicare beneficiaries are prove the opposite.
LTC Bullet: Progressive Bias Produces Regressive Policy,
February 2, 2024
LTC Comment: Public officials and their advisers prefer government
solutions to social problems, so their policies often produce deficient
outcomes.
LTC Bullet: “Dying Broke” Was Dead Wrong,
December 15, 2023
LTC Comment: Who knows more about long-term care (LTC) than KFF and the
New York Times? Answer: anyone who deals in facts and logic instead of
anecdotes and ideology.
LTC Bullet: You Pay for California’s LTC Profligacy and
Structural Racism, August 25, 2023
LTC Comment: California’s Medicaid program (Medi-Cal)
says come one, come all for free LTC, sends the bill to federal taxpayers,
and institutionalizes structural LTC racism. What’s happening?
LTC Bullet: The LTC Narrative,
June 30, 2023
LTC Comment: The dominant long-term care narrative crowds out inquiry,
critical reasoning and creativity leaving conformity and groupthink. We
explain.
LTC Bullet: AI on LTC, May 5,
2023
LTC Comment: Artificial intelligence (AI) is all the rage these days. Does
it help or hurt long-term care planning? We ask; AI answers; and we
respond.
LTC Bullet: WA Cares Repercussions,
October 28, 2022
LTC Comment: Washington State politicians and bureaucrats think they can
do LTC insurance better than private sector professionals. What could
possibly go wrong?
LTC Bullet: LTC Strawman,
September 30, 2022
LTC Comment: Disproving a claim no one has ever made contributes nothing
to a crucial conversation about who should qualify for Medicaid LTC
benefits, when and under what circumstances. We critique Marc A. Cohen and
Jane Tavares: “Are
Wealthy Older Adults who use Medicaid Opportunistically Accessing the
Program?,” Journal of Aging & Social Policy.
LTC Bullet: Biased LTC Scholarship Misinforms Policymakers,
September 2, 2022
LTC Comment: Government-funded, ideologically biased research causes bad
policy decisions, as we explain with this critique of Richard W. Johnson
and Melissa M. Favreault, “Economic Hardship and Medicaid Enrollment in
Later Life: Assessing the Impact of Disability, Health, and Marital Status
Shocks,” published by the U.S. Department of Health and Human Services
Office of the Assistant Secretary for Planning and Evaluation, January 31,
2021, https://aspe.hhs.gov/reports/economic-hardship-medicaid-enrollment-later-life#results.
LTC Bullet: Begging the LTC Question,
May 27, 2022
LTC Comment: Long-term care analysts routinely ignore, diminish and/or
misrepresent the impact of Medicaid planning (artificial
self-impoverishment to qualify for benefits) on the long-term care market.
Here’s an example taken from Richard W. Johnson and Melissa M. Favreault,
“Economic
Hardship and Medicaid Enrollment in Later Life: Assessing the Impact of
Disability, Health, and Marital Status Shocks,” HHS/ASPE/BHDAP,
January 31, 2021.
LTC Bullet: Moses vs. Grabowski on Long-Term Care,
February 25, 2022
LTC Comment: David
C. Grabowski, PhD, is Professor of Health Care Policy in the
Department of Health Care Policy at Harvard Medical School. Professor
Grabowski is omnipresent in the news about long-term care. Stephen
A. Moses is president of the Center for Long-Term Care Reform. His
media megaphone is more subdued. But both were featured yesterday in McKnight’s
Long-Term Care News. Their differing views on what ails long-term care
services and financing provide food for thought about this complicated
topic.
LTC Bullet: Long-Term Care’s Fundamental Fallacy,
February 18, 2022
LTC Comment: We explain the fundamental fallacy that leads LTC analysts
and policy makers astray.
LTC Bullet: The InLTCgentsia,
September 3, 2021
LTC Comment: Should LTC intellectuals, politicians and bureaucrats who pay
no price for being wrong direct long-term care financing reform?
Considerations follow.
LTC Bullet: WISHful Thinking,
August 20, 2021
LTC Comment: Hope springs eternal among the LTC anointed that one more
government program forced on the public at the expense of the productive
economy can reduce the damage done by its many failed predecessors.
Analysis of the WISH Act follows.
LTC Bullet: Milken Groupthink Fumbles LTC Financing,
April 16, 2021
LTC Comment: You might expect innovative ideas from the Milken Institute,
but when it comes to long-term care financing, all you get is ideological
retreads.
LTC Bullet: MACPAC Captured,
April 2, 2021
LTC Comment: Signs in the Medicaid and CHIP Payment and Access
Commission’s (MACPAC’s) estate recovery report point to its capture by the
Medicaid planning bar.
LTC Bullet: The Key to LTC, March
19, 2021
LTC Comment: Solving the long-term care financing crisis isn’t so hard if
you avoid ideology and take human nature into account. A better
public/private partnership is an easy and available solution.
LTC Bullet: Social Insurance is an Oxymoron,
February 5, 2021
LTC Comment: Insurance is individualistic, so “social insurance” is a
contradiction in terms. Meaning and consequences explained.
LTC Bullet: Spousal Impoverishment, Then and Now,
January 22, 2021
LTC Comment: The myth that access to Medicaid LTC benefits requires
impoverishment is pervasive. A dose of reality concerning spousal impoverishment
specifically follows.
LTC Bullet: Is Medicaid the LTC Solution or the Problem?,
December 4, 2020
LTC Comment: Will more Medicaid funding and regulation help (short-term)
and harm (long-term) America’s fragile long-term care system? Answers
follow.
LTC Bullet: Modern Monetary Theory and Long-Term Care,
October 23, 2020
LTC Comment: Finally, a solution for the long-term care financing crisis.
Or not? Explanation follows.
LTC Bullet: The Keystone Kops of LTC Insurance,
October 9, 2020
LTC Comment: What happens when the Keystone Kops design a long-term care
insurance plan? Answer: Washington State’s “Long-Term
Services and Supports Trust Act (Trust Act),” enacted in 2019.
LTC Bullet: How Not to Redesign Long-Term Care,
June 12, 2020
LTC Comment: Do we really need more government money and regulation for
long-term care, as this Forbes columnist insists? Analysis and
better choices follow.
LTC Bullet: Where Long-Term Care Went Wrong and How to Fix
It, January 3, 2020
LTC Comment: Officials and analysts attack the symptoms of long-term care
dysfunction (exploding costs, nursing home bias, and poor quality) without
addressing the cause (easy access to Medicaid for consumers and strong
incentives for states to maximize federal Medicaid matching funds).
Everything follows from that observation.
LTC Bullet: The Battle Lines Are Drawn,
October 25, 2019
LTC Comment: Two sides advocate diametrically opposite solutions for the
long-term care crisis. Who are they? What do they want? Which will win?
Answers follow.
LTC Bullet: To Fix Long-Term Care, Redefine the Problem,
September 27, 2019
LTC Comment: Recent research suggests long-term care is not the gargantuan
crisis previously thought. So, private sector solutions, including LTC
insurance, may be far more effective than commonly believed.
LTC Bullet: Why Too Little Home Care?,
June 28, 2019
LTC Comment: Why is home care so unaffordable and hence unavailable to so
many? Two views follow: more government money or better directing what we
already spend to encourage more private financing.
LTC Bullet: Middle Market Mayhem,
June 7, 2019
LTC Comment: LTC analysts, advocates, and providers are wringing their
hands about the middle market’s future inability to afford senior living.
We mitigate the problem and re-offer a 25-year-old solution.
LTC Bullet: Remember the Middle,
Friday, May 10, 2019
LTC Comment: A recent Health Affairs article accurately assessed
the plight of middle-income seniors whose resources will be inadequate to
fund their senior living and long-term care. But the article proposed
interventions that would exacerbate the problem.
LTC Bullet: Amplify LTC Sanity,
February 13, 2019
LTC Comment: In today’s echo chamber of irresponsible fiscal and monetary
advocacy, a voice for responsible LTC planning and policy is more critical
than ever. Join us!
LTC Bullet: How and How Much Medicaid Reduces Lifetime
Medical Spending for Affluent Retirees, October
10, 2018
LTC Comment: Medicaid is welfare, so of course it reduces lifetime medical
spending of the poor. But here’s evidence Medicaid radically reduces
medical spending by the affluent, especially for those savvy enough to
maximize “Medicaid planning.”
LTC Bullet: The New Fallacy of Impoverishment,
June 29, 2018
LTC Comment: Government should declare success in the War on Poverty and
eliminate policies that discourage personal responsibility and work.
LTC Policy Blinders, May 25, 2018
LTC Comment: We explain why and how LTC policy analysts evade facts that
contradict their predisposed positions in favor of compulsory government
LTC insurance.
Feder/Cohen Proposal Ignores LTC Problems’ Cause,
May 18, 2018
LTC Comment: We explain how government intervention caused the
dysfunctions in long-term care that Feder/Cohen seek to correct with more
government intervention, including institutional bias, poor access and
quality, excessive dependency on family caregiving, inadequate financing,
and lack of insurance.
LTC Evasion, May 11, 2018
LTC Comment: We explain what LTC scholars evade and why.
Feder Fantasy Fatally Flawed (Cohen Contribution
Notwithstanding), May 4, 2018
LTC Comment: A new Feder/Cohen proposal would take long-term care out
of the frying pan into the fire.
LTC Bullet: Retirement Confidence and Asset Spend Down,
April 27, 2018
LTC Comment: Two new EBRI studies shed light on how workers/retirees’
expectations and behavior differ.
LTC Bullet: Have Your Cake Until It Eats You,
March 23, 2018
LTC Comment: Americans want to have their cake (entitlements) and eat it
too, but trends show this cake will eat our economy first. Scary evidence
follows.
LTC Bullet: Is it Spend Down or Medicaid Planning?,
July 14, 2017
LTC Comment: A lot of what passes for Medicaid “spend down” in the
scholarly literature is really Medicaid planning. We explain and give
examples.
LTC Bullet: Medicaid, Home Ownership and
Long-Term Care Financing, July 7, 2017
LTC Comment: Medicaid’s estate recovery requirement induces aging
Americans to reduce home ownership, decrease home equity and set up trusts
in order to qualify for Medicaid long-term care benefits.
LTC Bullet: Home Equity and LTCI Demand,
June 30, 2017
LTC Comment: We explore the Professor Thomas Davidoff’s thesis that home
equity “substitutes” for long-term care insurance demand and suggested
instead that Medicaid’s large home equity exemption obviates LTCI demand
by eliminating home equity’s liability for long-term care costs.
LTC Bullet: Is it Really Hopeless to Reduce Medicaid LTC
Costs?, June 23, 2017
LTC Comment: Kaiser Family Foundation researchers despair of reducing
Medicaid LTC expenditures, but their “literature review” is incomplete,
misleading and risky.
LTC Bullet: The Broken Rhythm of Long-Term Care Reform,
May 19, 2017
LTC Comment: Why did Medicaid long-term care eligibility reforms quickly
follow economic recessions until the year 2000, but no longer? The answer
follows.
LTC Bullet: Hoist with its Own Petard
, April 28, 2017
LTC Comment: This Kaiser Family Foundation “Issue Brief” blows up its own
argument. We explain.
LTC Bullet: What’s Wrong with Bundled and Value-Based LTC
Payments? January 20, 2017 LTC Comment: Big
changes are afoot in government financing of post-acute and long-term
care--changes that will rattle private LTC financing options as well. We
present the big picture.
LTC Bullet: Medicaid LTC Data Insights,
October 14, 2016
LTC Comment: What’s happening with Medicaid LTC financing and why it
matters.
LTC Bullet: How Fiscal and Monetary Malfeasance Will Ruin
Long-Term Care, October 7, 2016
LTC Comment: Fiscal malfeasance ($20 trillion federal debt) enabled by
monetary malfeasance (artificially low interest rates) bode ill for the
economy and for Medicaid LTC financing. Here’s why and how.
LTC Bullet: Behind AHEAD,
September 2, 2016
LTC Comment: The people and organizations advocating a new, compulsory,
payroll-financed government program to fund catastrophic LTC expenses base
their arguments on dubious sources and reasoning. Details follow.
LTC Bullet: Half a Century of Bad Medicaid LTC Policy,
August 5, 2016
LTC Comment: Medicaid long-term care policy is a classic story of good
intentions leading to unfortunate consequences.
LTC Bullet: How the Government Ruined LTC (and We’ll Fix
It), June 10, 2016
LTC Comment: Government interference in the LTC marketplace since 1965
caused harmful unintended consequences that only clear analysis and bold
action can fix.
LTC Bullet: LTC at a Crossroads,
June 3, 2016
LTC Comment: Long-term care financing policy is at a critical crossroads
and may take a wrong turn. We explain.
LTC Bullet: Losing Principles,
April 29, 2016
LTC Comment: What’s happening to the basic principles of personal
responsibility and self-reliance that validate private insurance? We
reflect.
LTC Bullet: LTCI Defeatism,
April 1, 2016
LTC Comment: LTC insurance leaders should not surrender to
government-financed long-term care based on ideologically biased policy
analysis grounded in misleading data and fallacious arguments. We say
“Revolt!”
LTC Bullet: Three Cheers (But Two From the Bronx) for New
BPC-LTC Recommendations, February 5, 2016
LTC Comment: The Bipartisan Policy Center’s new report on long-term care
leads with LTCI (hear, hear!), but makes Medicaid even more tempting
(boo!) and adds a new, expensive, mandatory government program (boo!)
based on faulty premises. Our analysis and critique follow.
LTC Bullet: The Arrogance of LTC Analysts' Elitism,"
December 4, 2015
LTC Comment: Arrogance, ideological bias and elitism spoil the recent
research of abundantly endowed LTC analysts. We explain.
LTC Bullet: The Future of Long-Term Care Seen Through the
Prism of History, November 13, 2015
LTC Comment: Big changes are afoot in government financing of post-acute
and long-term care--changes that will rattle private LTC financing options
as well. We cover the big picture.
LTC Bullet: A New Revolution in Long-Term Care Financing .
. . by Government, November 6, 2015
LTC Comment: Radical, disruptive changes in how government pays for
long-term care are advancing rapidly. We provide background.
LTC Bullet: Another LTCI Hit Job?,
October 9, 2015
LTC Comment: What shall we make of this new attack on private long-term
care insurance? Answers follow.
LTC Bullet: Pandora Meets Rosy Scenario in CMS Projections,
July 31, 2015
LTC Comment: The aging demographic evils in Pandora’s “box” don’t find
their way into CMS actuaries’ health expenditure estimates for the coming
decade. Quotes and our comments follow.
LTC Bullet: New Data on LTC Incidence, Duration, Cost and
Financing Sources, July 24, 2015 LTC Comment:
New numbers, better than the old numbers, but they require further
clarification and explanation.
LTC Bullet: Holding CMS’s Feet to the Fire,
February 6, 2015
LTC Comment: When a federal agency fails to enforce the law hurting the
poor it’s supposed to help and costing tax payers billions of dollars,
bureaucratic heads should roll. Background and details follow.
LTC Bullet: When Bad Models Happen to Good People,
January 16, 2015, guest Bullet by Stephen D. Forman
LTC Comment: We offer the last word on that Boston College fiasco of poor
scholarship and bad economics.
LTC Bullet: How Careless Economists Boosted LTC Risk,
December 12, 2014
LTC Comment: We explain how Boston College economists generated poor
long-term care planning advice that national media unfortunately
amplified.
LTC Bullet: IG Report Reveals Medicaid Estate Recovery
Weakness, December 5, 2014
LTC Comment—A newly released USDHHS Inspector General report shows few
states do Medicaid estate recoveries well resulting in a potential annual
loss, we infer, of $2.5 billion. Details, numbers, and why it matters
follow.
LTC Bullet: IG Report Reveals Costly Medicaid Enforcement
Failures, November 21, 2014 LTC Comment--The
USDHHS Inspector General reports that many states failed to implement
mandatory provisions in OBRA ’93 and/or DRA ’05 designed to discourage
abuse of Medicaid LTC benefits. Details follow.
LTC Bullet: Does Medicaid Solvency Matter?,"
October 31, 2014
LTC Comment: CMS says Medicaid solvency “is not an issue.” We beg to
differ.
LTC Bullet: CMS Health Expenditure Data Mask LTC Cost
Growth, September 5, 2014
LTC Comment: CMS actuaries’ estimates of health expenditures for 2013-2023
downplay the big story, snowballing LTC costs. We explain.
LTC Bullet: Entitlement Double Talk,
August 1, 2014
LTC Comment: To read the major media coverage of the 2014 Medicare
Trustees report, you’d think things are looking up for the 49-year-old
mega-program. Think again.
LTC Bullet: GAO Punts on Medicaid Planning,
July 3, 2014
LTC Comment: Another GAO report underplays dramatic findings about the
role, methods and extent of Medicaid planning and loose LTC eligibility
rules.
LTC Bullet: Will Bipartisan LTC Policy Be Better?,
April 11, 2014
LTC Comment: Heads up! Consensus is coalescing around a bipartisan
long-term care financing solution. Let’s be hopeful, but wary.
LTC Bullet: Who Gets Medicaid LTC?,
March 28, 2014
LTC Comment: Is Medicaid a long-term care safety net for the poor, the
middle class, even the affluent, all of the above? Questions remain, but
answers abound.
LTC Bullet: WSJ Misfires on LTC Insurance,
February 14, 2014
LTC Comment: We dissect and correct a misbegotten column in the Wall
Street Journal.
LTC Bullet: PBS’s 6 LTC Tips Miss the Mark,
November 8, 2013
LTC Comment: What’s wrong with the conventional wisdom about how to
resolve America’s long-term care crisis?
LTC Bullet: The LTC Blind,
October 25, 2013
LTC Comment: “There are none so blind as those who will not see.” That
proverb applies perfectly to a recent column about long-term care by the
Urban Institute’s Howard Gleckman.
LTC Bullet: Medicaid Spend Down that Isn't and Why it
Matters," July 19, 2013
LTC Comment: Claiming “transitions” to Medicaid are evidence of
catastrophic LTC asset “spend down” misrepresents the truth and should be
publicly recanted. We answer who, what, when, where and why.
LTC Bullet: What Should the LTC Commission Do?,
June 21, 2013
LTC Comment: How should the LTC Commission prioritize its work and
recommendations? Some thoughts follow.
LTC Bullet: SCAN the LTC Possibilities,
April 5, 2013
LTC Comment: SCAN is a fountainhead of ideas about long-term care
financing, but are those ideas potable? We analyze.
LTC Bullet: Nursing Home Spend Down Misunderstood and
Late-Breaking LTCI Industry News,
July 20, 2012
LTC Comment: A recent EBRI study that claims nursing home stays are wiping
out Americans’ savings is based on a fallacy and mistaken. What’s really
happening?
LTC Bullet: Moses Replies to Congressman's Questions
(LTC Embed Report #11), October 13, 2011
LTC Comment: House Oversight and Government Reform Healthcare Subcommittee
ranking member Danny Davis (D, IL) asked me some questions in writing
after the 9/21 hearing on "Examining Abuses of Medicaid Eligibility
Rules." His questions and my answers follow.
LTC Bullet: Friendly Fire in the Class War
(LTC Embed Report #6), September 22, 2011
LTC Comment: Steve Moses's Congressional testimony on Wednesday was
well-received except for an ad hominem attack, "friendly fire" in
the class war. An explanation, witness testimonies, and a video of the
hearing follow.
LTC Bullet: CLASSless Journalism,
September 21, 2010
LTC Comment: Reporting only the CLASS program's dubious benefits and none
of its inevitable detriments is negligent journalism. An example follows.
LTC Bullet: New LTCI Report: Research or Propaganda?,
June 8, 2010
LTC Comment: Is a newly updated report on LTC insurance by the
Congressional Research Service really research, or CLASS Act propaganda?
You decide.
LTC Bullet: The Enemy of LTC Truth,
February 8, 2010
LTC Comment: Albert Einstein said "Unthinking respect for authority is the
greatest enemy of truth." See how this principle applies to long-term
care.
LTC Bullet: CLASS Consciousness,
October 21, 2009
LTC Comment: To hear Kaiser Family Foundation speakers, the CLASS Act is a
no-brainer for passage and implementation. We offer a wake-up call.
LTC Bullet: We Reply to Washington Post Blast at
Federal LTCI, August 14, 2009
LTC Comment: Read our reply to the Washington Post's "Federal
Diary" criticism of Federal LTCI's premium increase.
LTC Bullet: How Much More Wrong Can They Get It?!,
July 21, 2009
LTC Comment: Another "report" from the usual suspects gets long-term care
advice dead wrong.
LTC Bullet: KFF Misfires on LTCI,
June 9, 2009
LTC Comment: A new study of private long-term care insurance published by
the Kaiser Family Foundation fails in the usual, predictable ways. Details
follow.
LTC Bullet: LTC Clueless, May 26,
2009
LTC Comment: Consumers' denial of LTC risk and cost is nothing compared to
the naiveté of professionals who should know better.
LTC Bullet: New LTC Financing Study Uninterpreted or
Misinterpreted, March 24, 2009
LTC Comment: A new report on LTC financing by Avalere Health was reported
uncritically by many and mistakenly by one source.
LTC Bullet: We Critique WSJ on Medicaid Planning,
January 16, 2009
LTC Comment: Within 24 hours, we replied to a Wall Street Journal
column that promoted Medicaid planning for long-term care.
LTC Bullet: NYT Asks Medicaid Planner to Advise on LTCI,
July 18, 2008
LTC Comment: The New York Times added insult to injury by inviting
a notorious Medicaid planner to advise readers on private long-term care
insurance. We respond.
LTC Bullet: WSJ Attacks LTCI, We Respond,
February 26, 2008
LTC Comment: Today's front-page Wall Street Journal article
criticizing long-term care insurance was as one-sided and misguided as a
similar piece published by the New York Times also during a major
industry conference. We reply, same day, as follows.
LTC Bullet: Hillary Clinton on LTC,
January 3, 2008
LTC Comment: Presidential candidate Senator Hillary Clinton has promised a
cornucopia of LTC benefits if elected. Would our service delivery and
financing system be better or worse if she delivered? We comment.
LTC Bullet: The NY Compact: Analysis, Conclusions, and
Recommendations, July 31, 2007
LTC Comment: Is the New York Compact the future of long-term care
financing or the last gasp of an old, failed system?
LTC Bullet: Medicaid Estate Recover. . .up,
July 5, 2007
LTC Comment: Medicaid estate recovery could be a major source of non-tax
revenue for the ailing LTC safety net for the poor, but AARP would tie the
program in bureaucratic knots.
LTC Bullet: GAO on LTCI Partnerships,
June 20, 2007
LTC Comment: GAO drops the ball again on the issues of Medicaid, long-term
care financing and private insurance.
LTC Bullet: GAO AWOL on LTC TOA,
May 2, 2007
LTC Comment: The Government Accountability Office has again displayed
stunning miscomprehension of the Medicaid eligibility, Medicaid planning
and transfer of assets issues.
LTC Bullet: Take Georgetown's Facts With a Big Grain of
Salt, February 15, 2007
LTC Comment: Three new "fact sheets" from the Georgetown LTC Financing
Project are spoiled by ideological bias. This Bullet critiques
Medicaid's Spousal Impoverishment Protections (February
2007) ,
Medicare and Long-Term Care (February 2007)
and
National Spending for Long-Term Care (February 2007)
LTC Bullet: The DRA Bullets,
January 9, 2007
LTC Comment: Two Medicaid planners lament the DRA we praised and defended
in 21 LTC Bullets last year. Their whining, our replies plus links
to all the DRA Bullets follow.
LTC Bullet: Medicaid Commission Errs by Omission,
August 9, 2006
LTC Comment: The national Medicaid Commission, appointed last year to fix
Medicaid (including its dysfunctional LTC component) before the welfare
program implodes financially, is way off track.
LTC Bullet: Kaiser Cover-Up Continues,"
April 27, 2006
LTC Comment: Urban Institute "scholars," aided and abetted by the Kaiser
Family Foundation, employed an underhanded straw man argument in the
foundation's latest unsuccessful attempt to debunk the impact of Medicaid
planning abuse.
LTC Bullet: Microsimulate This!,
March 28, 2006
LTC Comment: The fundamental things apply as time goes by--like "garbage
in, garbage out." Take for example a recent Inquiry article that
estimates future public and private LTC costs. Our critique follows.
LTC Bullet: LTC Victory, February
2, 2006
LTC Comment: The Deficit Reduction Act of 2005 passed yesterday curbing
Medicaid abuse and unleashing LTC Partnerships. Celebrate? Sure. But don't
take a victory lap until you consider what can go wrong.
LTC Bullet: Georgetown, GAO and Kaiser: The Bermuda
Triangle of Good LTC Policy, January 25, 2006
LTC Comment: LTC doubletalk is not the exclusive province of Medicaid
planners and AARP lobbyists. Otherwise often reliable analysts get
long-term care policy wrong too.
LTC Bullet: NPR Defends Medicaid Planning, Attacks
Messenger, January 4, 2006
LTC Comment: National Public Radio's "All Things Considered" show
took a slanted swipe at responsible Medicaid reform yesterday while
defending Medicaid planning abuse. Hear the broadcast version, followed by
our side of the story.
LTC Bullet: GAO on TOA Underwhelms,
October 5, 2005
LTC Comment: The Government Accountability Office's new report on Medicaid
asset transfers asks the wrong questions, uses the wrong data, and so
provides few helpful answers.
LTC Bullet: Alzheimer's Association Shortsighted on LTC
Financing, July 6, 2005
LTC Comment: The Alzheimer's Association's public position on Medicaid
reform and long-term care financing is a classic example of how good
intentions invite unintended consequences.
LTC Bullet: LTC Bombshell, June
29, 2005
LTC Comment: Results from a poll of state Medicaid programs by a
Congressional office with subpoena power may blow the lid off a carefully
orchestrated cover-up of Medicaid planning abuses. Lists, summarizes and
analyzes studies that pooh-pooh Medicaid planning.
LTC Bullet: Where There's Smoke, There's Fire,
May 18, 2005
LTC Comment: Our critique follows of "Medicaid's coverage of nursing home
costs: Asset shelter for the wealthy or essential safety net?" by Ellen
O'Brien of the Georgetown Long-Term Care Financing Project.
LTC Bullet: Medicaid Planners Confess,
October 2, 2003
LTC Comment: A survey intended to exonerate Medicaid planners is actually
the strongest indictment of artificial impoverishment yet.
LTC Bullet: "Nursing Home Care Virtually Free For Life,"
Tuesday, May 7, 2002
LTC Comment: What follows is a transcription of excerpts from a
professionally produced and mass-distributed videotape from a man and his
company who promise lifelong free long-term care.
LTC Bullet: They're Baaaack . . . Medicaid Planners Rise
Again, April 25, 2001
LTC Comment: Ever since Congress and then-President Bill Clinton nailed
them with mandatory estate recovery (OBRA '93), "Throw Granny in Jail" (HIPAA
'96) and "Throw Granny's Lawyer in Jail" (BBA '97), the Medicaid estate
planning attorneys have laid low. No longer.
LTC Bullet: More Bad Advice from Consumer Reports,
November 15, 1999
LTC Comment: Individuals and organizations most critical of private
long-term care insurance are usually the ones lining their pockets with
Medicaid estate planning profits.
#############################
Updated Monday, February 17, 2025,
10:03 AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-006:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
The Biggest Health Policy Decisions Now
Facing the Trump Administration
-
Reverse mortgages could be ‘practical’
long-term care funding option
-
Responsible Governing Involves Making Tough
Decisions – Here’s a Guide
-
Think Bigger: Meaningful Health Reform
-
US voters overwhelmingly support caregiver
tax credit: survey
-
Report: Prevalence of older Americans
without disabilities rose between 2008 and 2017
-
Sneak Peek of Long Term Care Success
-
How to Avoid Medicaid Estate Recovery
-
The Health Wonk Shop: What’s Next for the
Affordable Care Act?
-
ILTCI Session Matrix
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Monday, February 10, 2025,
10:03 AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-005:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Losing Focus: How the ACA’s Medicaid Expansion Left
Traditional Enrollees Behind
-
Number of family caregivers helping older adults
with dementia surged over 11-year span: study
-
The care crisis: Eldercare collides with childcare
-
Lawmakers push Trump to block Medicaid 80/20 rule
-
ILTCI Conference to Screen Powerful Caregiving
Documentary at 2025 Keynote
-
The Nation's Fiscal Health: Strategy Needed as Debt
Levels Accelerate
-
U.S. Short-Term Care Insurance Market to Reach
$110.1B by 2033
-
New report details financial, emotional toll of
Parkinson’s on family caregivers
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Friday, February 7, 2025,
10:03 AM (Pacific)
Seattle—
#############################
LTC BULLET: MEDI-CAL’S
ASSET TEST ELIMINATION
LTC Comment: We explore
the topic of California’s Medicaid program (Medi-Cal) eliminating the
asset test for long-term care benefit eligibility after the ***news.***
***
ILTCI ’25 Conference announced a special screening of excerpts from
Caregiving,
a compelling, two-hour documentary executive produced by Bradley Cooper
and produced by Lea Pictures, Ark Media, and WETA, scheduled to air in
primetime on more than 330 PBS stations nationwide in June 2025. This
groundbreaking public media documentary delves into the personal stories
of caregivers, shedding light on the challenges they face in providing
short and long-term care, as well as palliative and end-of-life care for
individuals of all ages. Join us March 10, 2025, from 9:00 - 10:15 am ET
for the Caregiving Keynote Presentation, Sponsored by
CareScout. ***
*** DOGE (the ad hoc,
but influential “Department of Government Efficiency”) claims to have
already cut over $64 billion according to the
National Debt Clock. GAO says more is needed to address “our
unsustainable fiscal path” as we reported in this LTC Clipping.
Center for LTC Reform premium members receive LTC Clippings by
email in real time. Regular members receive the same content compiled in
weekly LTC E-Alerts.
Join the Center, receive these publications, and help us change LTC
financing policy for the better.
2/5/2025, “The
Nation's Fiscal Health: Strategy Needed as Debt Levels Accelerate,” by
GAO, GAO-25-107714
Quote: “The
federal government is on an unsustainable fiscal path that poses serious
economic, security, and social challenges.
We reported that:
-
As of September 30,
2024, publicly held debt was $28.2 trillion, or 98% of the size of the
economy
-
Publicly held debt is
projected to grow more than twice as fast as the economy, reaching 200%
of the size of the economy by 2047
-
Government spending on
net interest in FY 2024 exceeded federal spending on Medicare and
national defense, and is projected to keep growing
We continue to recommend
that Congress develop a strategy to inform the difficult policy choices in
addressing our unsustainable fiscal path.
For more information on
federal debt, see our resource: How
Could Federal Debt Affect You?”
LTC Comment:
Another dire warning from the Government Accountability Office (GAO).
Likely to have the same impact as all the previous ones. Namely, none. Can
the unofficial Department of Government Efficiency (DOGE) do better?
According to the
National Debt Clock, DOGE has already cut over $60 billion. As Reagan
said, “Trust, but verify.” We’ll see what’s real, if anything, in time.***
LTC BULLET: MEDI-CAL’S
ASSET TEST ELIMINATION
LTC Comment: I’m
researching Medi-Cal’s elimination of the asset test for LTC benefit
eligibility. Before I put all the pieces together into an organized
analysis, I thought readers might like to see some of the information I’m
turning up. Following is a sampling with sources linked. Click through for
eye-opening insights into the mind-boggling, budget-busting ideology
behind this momentous policy change.
“As of January 1, 2024,
Medi-Cal will no longer count assets to determine eligibility. This
means that anyone, regardless of how much they own, may receive Medi-Cal
benefits, including:
- Individuals
in skilled nursing or intermediate care facilities or those who qualify
for home and community based services
- People who
are 65 or over, blind or disabled
- Low-income
persons with dependent children
- Children
under 21
- Pregnant
women
“SSI and other
categorically-related recipients are also automatically eligible for Medi-Cal.”
(Overview
of Medi-Cal for Long Term Care by
California Advocates for Nursing Home Reform,
emphasis added)
“Asset Elimination
Overview
• Assembly Bill 133 (Chapter 143, Statutes of 2021) was signed into law by
the Governor on July 27, 2021. This law included a two-phased approach to
eliminating the asset test used to determine eligibility for NonModified
Adjusted Gross Income (Non-MAGI) Medi-Cal Programs.
• Phase I, implemented on July 1, 2022, increased asset limits for all
NonMAGI programs to $130,000 per individual and $65,000 for each
additional household member (up to 10).
• Phase II, effective on January 1, 2024, will eliminate the asset test
entirely for Non-MAGI “Medi-Cal programs, including Long-Term Care and
Medicare Savings Programs.”
(From
webinar for “advocates”)
“Q: For which Medi-Cal
programs will the asset limit be eliminated?
All non-expansion Medi-Cal programs, including Aged, Blind, and Disabled,
Medi-Cal with a Share of Cost, 250% Working Disabled Program, long-term
care, and Medicare Savings Programs (MSPs). MSPs include four specific
programs: Qualified Medicare Beneficiary (QMB), Specified Low-Income
Medicare Beneficiary (SLMB), Qualified Income (QI), and Qualified Disabled
Working Individual (QDWI) programs. The MSPs help low-income Medicare
enrollees pay for Medicare out-of-pocket expenses including premiums and
cost-sharing. (Note: those enrolled in Medi-Cal expansion already do not
have an asset limit).”
(Justice
in Aging)
“As Medi-Cal coverage is
an essential lifeline in providing for the health care needs for millions
of beneficiaries (including dental, vision, hearing, transportation, and
long-term care), this win [elimination of the asset test] greatly
increased the quality of life, health and economic wellbeing of tens of
thousands of people.” (California
Health Advocates, emphasis added)
“Starting January 2024,
there will no longer be an asset limit for Medi-Cal eligibility.
This change has significant implications, as it means that more
individuals can now qualify for Medi-Cal and access home care services through
the In-Home Supportive Services Program.” (Bet
Tzedek, emphasis in the original)
“Some 36% of
Californians are covered by Medicaid, compared with 19% of Floridians and
15% of Texans. The federal share of the Golden State’s Medicaid
spending—nearly $120 billion—is more than Florida’s entire budget.” (WSJ
column)
“Consider California,
where 37% of residents are covered by Medicaid. The state has extended
Medicaid to undocumented immigrants and waived asset limits for
beneficiaries. Mr. Newsom’s budget forecasts some $190 billion in Medicaid
and other health spending this year, $119 billion of which will be picked
up by the feds. The latter amount is greater than Florida’s annual
budget.” (Wall
Street Journal editorial, 1/24/25)
“A [transfer of assets]
lookback period will no longer apply to transfers made on or after January
1, 2024.” (Overview
of Medi-Cal for Long Term Care by
California Advocates for Nursing Home Reform)
“Medi-Cal applicants,
beneficiaries and their spouses should always be aware of the Medi-Cal
Recovery rules and plan ahead if they want to avoid recovery on their home
or other assets. For detailed information on the Medi-Cal Recovery
program, see CANHR’s consumer booklet on Medi-Cal Recovery, https://canhr.org/wp-content/uploads/Medi-Cal_Recovery.pdf”
(Overview
of Medi-Cal for Long Term Care by
California Advocates for Nursing Home Reform)
“A new
report from the Kaiser Family Foundation finds that nursing home
staffing has decreased from 2015-2024 and the number of federal
deficiencies assessed per facility has increased. The KFF data show that
staffing in California nursing homes has decreased from 4.54 hours of
nurse staff per resident per day to 4.39 while the number of deficiencies
per facility has risen from 10.5 to a whopping 16.7. Also from 2015 to
2024, the percentage of California nursing homes receiving a deficiency
for actual harm or jeopardy nearly doubled, from 14% to 27%.”
(Staffing
Down, Deficiencies Up in Nursing Homes Throughout the U.S.)
“Recent Surge in
Senior Caseload Driving Increase in Costs. From January 2024
through July 2024, we have observed a sharp increase in Medi-Cal
enrollment among the senior population. Specifically, monthly growth
averaged about 14,500 people, notably higher than the previous six months
(averaging 1,600) or even during the continuous coverage period (averaging
6,200), when the state temporarily paused redeterminations of enrollee
eligibility. We assume that the key driver of this caseload surge is the
recent (January 1, 2024) full elimination of the asset limit test. (In
addition to specific income limits, prior to July 2022, seniors and
persons with disabilities faced strict asset limits for eligibility.
Specifically, nonexempt assets could not exceed $2,000 for individuals and
$3,000 for couples. The 2021 budget package raised the asset limit to
$130,000 for individuals and $195,000 for couples effective July 2022, and
fully eliminated the asset test as of January 1, 2024.)” (From November
20, 2024,
The 2025‑26 Budget: Medi-Cal Fiscal Outlook)
“As a result of the
terms of the ACA’s expansion of Medicaid, the federal government currently
discriminates against traditional Medicaid enrollees. With expansion, Medicaid
resources have been diverted from children and individuals with
disabilities to able-bodied, working-age adults. And existing
Medicaid enrollees have a harder time obtaining health care appointments
after expansion, with a
large increase in emergency department use for non-emergency services.”
(Source)
“Skilled nursing
facility residents must agree to pay the facility a portion of their
income each month. This is called the monthly resident cost and is treated
much like rent. The resident is responsible for paying their monthly
resident cost to the facility, and Medi-Cal will then cover the remaining
costs for the month. …
“For example, under a
legal settlement, Hunt v. Kizer, recipients may use old, unpaid
medical bills that they have to reduce the monthly Medi-Cal resident cost.
Original documentation showing the billing statement is an outstanding
balance should be provided to the County eligibility worker. … The monthly
resident cost will be adjusted to reflect the cost of the outstanding
balance, which could, for example, mean no monthly resident cost until the
old, unpaid bills are paid off. This is not automatic and should be
discussed with the Medi-Cal county eligibility worker.
“Under the Johnson
v. Rank settlement, recipients may use their monthly resident cost to
pay for medically necessary supplies, equipment or services not covered
under the Medi-Cal program. This deduction is only applicable to long term
care residents.”
(Overview
of Medi-Cal for Long Term Care by
California Advocates for Nursing Home Reform)
#############################
Updated Monday, February 3, 2025,
10:03 AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-004:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
- Spending on home healthcare grows twice as fast as total personal
healthcare spending over past 18 months
- Dealing with our Dickensian long-term care system
- Waterlily, a startup using AI to predict long-term care needs,
clinches $7M in seed round
- The U.S. Has Reached The Peak Of Peak 65
- Providers shaken by flip-flops, uncertainty as White House attempts
broad freeze on federal spending
- CMS goes after nursing homes’ third-party pay policies with updated
guidance
- Crisis in Long-Term Care Insurance: Financial Situation Reaches
Critical Levels
- People with family who need long-term care more likely to plan for
their own potential assisted living expenses, survey finds
- Long-term care continues to lead in healthcare bankruptcies
- U.S. Short-Term Care Insurance Market to Reach USD 110.1 Billion by
2033 - Persistence Market Research
- Medicare Advantage Enrollment Has Surged. Big Savings for
Beneficiaries Help Explain Why
- Revisions to WA Cares: What SB 5291 gets right and what it misses
- Ask the Hammer: Secure Act 2.0: New Long-Term Care Funding Option
- Medicaid Applicants: Protecting Your Healthy Spouse in 2025
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated
Monday, January 27, 2025, 10:03 AM (Pacific)
Seattle—
#############################
LTC Comment: “Statistics don’t lie, but liars use
statistics.” Still! We explain after the ***news.***
*** ICYMI: Read this latest of our 23-year annual
series as context for today’s LTC Bullet: “SO
WHAT IF THE GOVERNMENT PAYS FOR MOST LTC, 2023 DATA” ***
*** 1/17/2025, “Where
did the private payers go?,” by Stephen A. Moses, McKnights LTC
News
Quote: “Bottom line, CMS sold LTC providers a
bill of goods. Medicaid demands Ritz Carlton care but pays Motel 6 rates.
It converts profitable private pay revenue into reimbursements too low to
sustain providers, much less finance quality care. The major trade
associations representing nursing homes should mobilize to demand
market-based payment rates from Medicaid. That would eliminate both the
current inadequate Medicaid rates and the excessively high private rates
required now to compensate for Medicaid losses. It would also end the
caregiver shortage by enabling providers to pay competitive wages.”
LTC Comment: The current, Medicaid-based
financing system for nursing homes is unconscionable. Nothing is being
done to fix it. Most of the usual proposals for LTC financing reform would
only make the situation worse. Some of us are working on a new approach to
revolutionize the LTC market. Stay tuned. ***
LTC BULLET: LTC DATA MANIPULATION II
LTC Comment: We published “LTC Bullet:
LTC Data Manipulation" on August 30, 2024. In the meantime, new 2023
data have become available that make our point about KFF’s and CMS’s
misinterpretation and manipulation of LTC data even more forcefully. So we
offer the same analysis again below, but using the latest 2023 NHE data
National Health Expenditure data on long-term care (LTC) spending seem
straight forward. Three NHE tables cover expenditures for Nursing
Facilities and Continuing Care Retirement Communities (CCRCs) (Table 15),
Home Health Care Services (Table 14) and Other Health, Residential and
Personal Care Services (Table 13). Endnotes 1, 2, and 3 below describe
those categories, respectively. We provide summary tables following our
commentary that include all these spending sources for 2023 and 2022 data.
They cover the LTC waterfront, but KFF (Kaiser Family Foundation) says
they need some adjustments.
For example, in “10
Things About Long-Term Services and Supports (LTSS),” published July
8, 2024, KFF explains that it “excludes spending from certain payers.”
These excluded sources include “Medicare spending [$100.3B in 2023], most
of which is post-acute care, but some of which is home health spending
that might be considered LTSS.” Also “excluded is spending from private
insurance [$59.7B in 2023] because much of those expenditures are for
rehabilitation and not LTSS.” Private long-term care insurance is excluded
“in most cases” because it “reimburses people for the expenses they pay
out-of-pocket and would be classified as out-of-pocket spending in the NHE
data.”
Backing out those sources has the effect of reducing
total LTC spending in 2023 from the $629.3 billion reported by NHE to
KFF’s $469.3 billion, 25 percent less. Let’s ask two questions. First, is
there a rationale for leaving those sources in the total instead of
excluding them? Yes. Take Medicare’s $100.3 billion for example. Of course
Medicare doesn’t pay for LTC, but it is critical to America’s LTC
financing system. LTC providers are heavily dependent on Medicaid which
pays them 70 percent of private-pay rates on average and often less than
the cost of providing the care. They survive financially only because
Medicare pays more generously for a much smaller number of sub-acute and
rehabilitation patients. Remove Medicare’s $100.3 billion and the whole
financing system collapses. To see the complete LTC financing picture
accurately, Medicare must be included in the total.
What about private insurance, including LTC
insurance? True, some health insurance benefits, such as major medical
coverage, go for rehabilitation, not LTC. But as in the case of Medicare,
those payments help sustain a rickety LTC service delivery system, so they
should not be excluded. For private LTC insurance specifically, isn’t it
interesting that it gets lumped into the “out-of-pocket” bucket. Why might
that be? That brings us to our second question.
Why do analysts and policymakers define LTC spending
in some ways and not in others? What effect do the exclusions just
described have on the big picture of LTC spending? Backing out Medicare
and private insurance raises Medicaid’s contribution to total LTC costs
from 44.2 percent in the table to 59.3 percent based on KFF’s reasoning.
It increases out-of-pocket spending from 12.9 percent in the table to
KFF’s 17.4 percent. In other words, these exclusions make Medicaid and
out-of-pocket expenditures appear much higher. Giving that impression
supports a specific policy agenda, what I’ve called the
LTC Narrative. Specifically, that narrative is that LTC costs are
impoverishing people all across America and driving up Medicaid
expenditures excessively which is why, according to the narrative, we need
a new, compulsory, payroll-funded LTC entitlement program.
KFF isn’t the only group pushing that agenda by
tinkering with the data. In 2011, the Centers for Medicare and Medicaid
Services (CMS) changed the definition of NHE categories to combine CCRCs
with nursing homes. That created an apples/oranges problem. Nursing homes
rely mostly on Medicaid and have few private payers. CCRC’s include mostly
private payers for independent and assisted living. They have fewer
nursing home residents and very little Medicaid. So this definitional
change had the effect of dropping Medicaid’s share of spending for the
category from over 40 percent in 2008 to under one-third (32.8 percent) in
2009. Back then, cutting costs was a priority. Likewise, this change drove
out-of-pocket expenditures up to over one-quarter, below what they would
be for CCRCs but far above what they would be for nursing homes. Making
out-of-pocket expenditures look high supports the narrative of widespread
catastrophic spend down and the demand for more government funding and
regulation.
The tables below give a more accurate rendering of
the LTC financing landscape. They show that when we leave in the funding
sources KFF excludes, out-of-pocket costs clock in at only 12.5 percent in
2022, 12.9 percent in 2023. But those figures still overstate the impact
of out-of-pocket LTC funding. Half of it is spend down of income, mostly
from Medicaid recipients’ Social Security benefits. Only half, or about
six percent, could come from savings. The vast majority of all LTC
financing comes from third-party payors, mostly government. Out-of-pocket
costs are nominal despite the widespread belief that Medicaid requires
impoverishment and families across the country are being devastated by LTC
costs. That lie is the real reason most people do not think about or plan
for LTC and end up on public assistance. It is no reason to compound the
error of relying too heavily on government funding and regulation by
adding more of the same with a big new entitlement program.
There is much more to this story. To understand what
is really wrong with LTC and what needs to be done to fix it, read the
Paragon Health Institute’s “Long-Term
Care: The Problem” and “Long-Term
Care: The Solution,” watch this “virtual
LTC event” featuring age wave visionary Ken Dychtwald and leading LTC
researchers and check out “Medicaid's
$100+ Billion Leak.”
Source:
National Health Expenditures*
|
2023 (Billions) |
Total |
Medicaid |
Medicare |
Priv Insur |
OOP |
Other Payers |
|
NH + CCRC |
211.3 +10.5%
100% |
64.2 +9.7%
30.4% |
44.0 +4.3%
20.8% |
20.6 +13.2%
9.7% |
55.1 +14.1%
26.1% |
27.4 +13.7%
13.0% |
|
HH |
147.8 +11.2%
100% |
51.2
34.6% |
51.8
35.0% |
21.5
14.5% |
17.7
12.0% |
5.6
3.8% |
|
Other |
270.2 +9.6%
100% |
162.8
60.3% |
4.5
1.7% |
17.6
6.5% |
8.9
3.3% |
76.3
28.2% |
|
Total |
629.3 +10.3%
100% |
278.2 +9.2%
44.2% |
100.3 +6.8%
15.9 % |
59.7 +13.3%
9.5% |
81.7 +14.3%
12.9% |
109.3 +11.6%
17.4% |
|
2022 (Billions) |
Total |
Medicaid |
Medicare |
Priv Insur |
OOP |
Other Payers |
|
NH + CCRC |
191.3
100% |
58.5
30.6% |
42.2
22.1% |
18.2
9.5% |
48.3
25.2% |
24.1
12.6% |
|
HH |
132.9
100% |
46.9
35.3% |
47.5
35.8% |
18.6
14.0% |
15.4
11.6% |
4.5
3.5% |
|
Other |
246.5
100% |
149.3
60.8% |
4.2
1.7% |
15.9
6.4% |
7.8
3.2% |
69.3
28.1% |
|
Total |
570.7
100% |
254.7
44.6% |
93.9
16.5% |
52.7
9.2% |
71.5
12.5% |
97.9
17.2% |
* Note that CMS changed the definition of National Health
Expenditure Accounts (NHEA) categories in 2011, adding for example
Continuing Care Retirement Communities (CCRCs) to Nursing Care Facilities.
This change had the effect of reducing Medicaid's reported contribution to
the cost of nursing home care from over 40% in 2008 to under one-third
(32.8%) in 2009. CMS also created a new category called "Other Third Party
Payers" (7.1%) which includes "worksite health care, other private
revenues, Indian Health Service, workers' compensation, general
assistance, maternal and child health, vocational rehabilitation, other
federal programs, Substance Abuse and Mental Health Services
Administration, other state and local programs, and school health." For
definitions of all NHEA categories, see
http://www.cms.gov/NationalHealthExpendData/downloads/quickref.pdf.
Nursing Care Facilities and
Continuing Care Retirement Communities:
Covers nursing and rehabilitative services
provided in freestanding nursing home facilities. These services are
generally provided for an extended period of time by registered or
licensed practical nurses and other staff. Care received in state & local
government facilities and nursing facilities operated by the U.S.
Department of Veterans Affairs are also included. These establishments are
classified in NAICS 6231-Nursing Care Facilities and NAICS
623311-Continuing Care Retirement Communities with on-site nursing care
facilities.
#############################
Updated Tuesday, January 21, 2025,
10:03 AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-003:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
-
Feds reject providers’ claims of ‘impossible’
standards in last push to defend nursing home staffing mandate
-
As Congress Looks to Reduce Federal Spending,
Medicare and Medicaid Remain Broadly Popular, and At Least Twice as Many
People Want to Increase Spending Rather Than Cut It
-
Protecting What Matters
-
Where did the private payers go?
-
Study: Medicare Advantage users largely in the dark
about dental, vision, hearing benefits
-
Baby boomers aim to stay put as political climate
drives others to contemplate moving in 2025
-
How do Medicaid Home Care Programs Support Family
Caregivers?
-
GAO Cites Overlap, Fragmentation of Agency Programs
for Older Adults
-
Combating rising premiums by addressing social
determinants of health
-
Under Trump, Medicaid Faces a 'Reset Moment'
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
Updated Monday, January 13, 2025,
10:03 AM (Pacific)
Seattle—
#############################
LTC
E-ALERT #25-002:
LTC NEWS AND COMMENT
LTC
Comment: Do you spend hours searching the internet for useful articles,
key data, and relevant reports to keep you on the forefront of
professional knowledge? Do you lose business because you’re blindsided by
clients or competitors who learn critical information before you do?
Here’s an antidote:
LTC
Clippings: The Center for Long-Term Care Reform notifies subscribers to
our LTC Clippings service daily of information you need to know. Each
message contains only the critical facts about new publications: a title,
representative quote, a link to the original, and our analysis in a
sentence or two. To inquire or subscribe, contact Damon at 206-283-7036
or
damon@centerltc.com.
Read testimonials by satisfied subscribers
here.
To subscribe online, please click
here.
LTC
E-Alerts: Once a week, we compile our daily LTC Clippings into a summary,
email it to Center for Long-Term Care Reform members, and archive it in
The Zone, our password-protected members-only website. Center members
also receive our weekly LTC Bullet op-ed. To join the Center and receive
all these benefits and more, contact Damon at 206-283-7036 or
damon@centerltc.com.
We no
longer post our LTC E-Alerts on the Center’s public access website, but
here’s what today’s LTC E-Alert contained: links, quotes and comments on
the following articles, reports, or data:
- CMS proposes MA payment increase of 4.3 percent for 2026
- Here's How Many Years You Can Expect to Live After Dementia
Diagnosis
- Trump presidency brings ‘mixed bag’ of regulatory wins, payment
fears: McKnight’s 2025 Outlook, Part 3
- [Updated] CMS program to offer RNs up to $50K each to work in
nursing homes
- National Health Expenditure Projections, 2023–32: Payer Trends
Diverge As Pandemic-Related Policies Fade
- Slowdown in household growth, housing demand anticipated, except for
those 80+
- What We’ve Learned About Dementia’s Toll on Family Finances
- Senior living represented among 300+ groups imploring Congress to
protect Medicaid as ‘backbone’ of health system
#############################
"LTC E-Alerts" are
a feature
offered by the Center for Long-Term Care Reform, Inc. to members at the
$150 per year level or higher. We'll track and report to you news and
analysis regarding long-term care financing, service delivery, and
research. We hope The LTC E-Alerts will help you attain and maintain a
high level of knowledge and competency in this complex field. The
Center for Long-Term Care Reform, Inc. is a private institute dedicated to
ensuring quality LTC for all Americans (www.centerltc.com).
#############################
|
LINKS
Here are some links
you can check out to find
valuable information on long-term care providers, financiers and insurers.
This is just for starters.
We'll add many more as time goes on plus advice on what to look for on
their sites.
www.ahca.org American Health Care Association
www.leadingage.org
American Association of Homes and Services for the Aging
www.alfa.org
Assisted Living Federation of America
www.nic.org
National Investment Center
www.ahip.net America's Health Insurance Plans
ltcconsultants.com Phyllis
Shelton's website
www.aaltci.org American Association for Long-Term Care
Insurance
ltcconnection.com
LTCi producers' information
www.ltcsales.com
LTCi Sales Strategies
www.ahia.net
Association of Health Insurance Advisors
|


